Vaccine Democide: Terrifying Data From Group Life Mortality Survey and Recent MIT Study
How many more have to die?
U.S Group Life Insurance Mortality Survey Reveals Terrifying Excess Mortality Data
page 23
Moderators: Elvis, DrVolin, Jeff
![]() by stickdog99 » Thu May 12, 2022 4:02 pm
by stickdog99 » Thu May 12, 2022 4:02 pm
![]() by Harvey » Thu May 12, 2022 6:33 pm
by Harvey » Thu May 12, 2022 6:33 pm
https://childrenshealthdefense.org/defender/germans-severely-injured-covid-vaccines/
500,000 Germans Severely Injured by COVID-19 Vaccines, Survey by Top Hospital Shows
Researchers at Charité Berlin, Germany’s top hospital and one of Europe’s largest, announced a high rate of COVID-19 vaccine severe side effects lasting months or longer based on a survey of about 40,000 Germans.
By Josh Guetzkow, Ph.D.
Researchers at Charité Berlin, Germany’s top hospital and one of Europe’s largest, announced a high rate of COVID-19 vaccine severe side effects lasting months or longer based on a survey of about 40,000 Germans.
Some highlights:
1. Researchers estimate eight serious side effects per 1,000 vaccinated people, compared to 0.2 estimated by the Paul Ehrlich Institute (PEI), Germany’s vaccine watchdog.
2. This equates to an underreporting factor (URF) of 40x, which is almost exactly the same as the Vaccine Adverse Event Reporting System (VAERS) URF estimated by Steve Kirsch.
3. The study’s lead researcher, Dr. Harald Matthes, estimated half a million Germans experienced serious side effects following vaccination. Survey findings indicate up to 80% of people with severe reactions recover within three to six months, but for 20% the symptoms persist.
This equates to 100,000 Germans currently suffering from long-term serious side effects. That means 0.16% of people vaccinated are still suffering serious side effects more than six months following vaccination.
4. This is a major embarrassment for the PEI, which has maintained all along that it is doing a thorough tracking of vaccine adverse events and denounced as “anti-vaxxers” anyone who questioned the official numbers.
5. Matthes called on the government to take people claiming vaccine injury seriously and to provide dedicated outpatient care to the vaccine-injured.
He noted most have been unable to find help in the current medical climate, which both strongly discourages talking about vaccine injury and is basically clueless about how to help the vaccine-injured.
Matthes also called for allowing doctors to discuss vaccine injury openly so that they can develop treatments without fear of being denounced as “anti-vaxxers.”
6. Matthes noted a strong similarity between many of the symptoms of so-called “long COVID” and vaccine injury and believes treatments for long COVID may be helpful in addressing vaccine injury.
For more on this, see my presentation at PANDA’s open science meeting on a unified theory of susceptibility to COVID and injuries from COVID-19 vaccines.
7. Germany set up outpatient clinics devoted to long COVID, and the vaccine-injured can turn to them for help. But there’s a problem: too many injuries.
From this article:“The special outpatient clinic at the University Hospital in Marburg is a prominent example of this. The employees actually wanted to do research on Long Covid, but now they mainly care for patients with severe vaccination side effects.
“Between 200 and 400 e-mails from those affected are now received daily in the Marburg special outpatient clinic, and the waiting list includes around 800 patients.
“The problem here, however, is that demand far outstrips supply. ‘We need more outpatient clinics, they are far from enough,’ emphasizes Matthes in the MDR report. [Note that outpatient treatment in German is machine-translated into ‘ambulances’ in English.]”
8. This story is huge. It is akin to researchers at Harvard Medical School coming forward and announcing the Centers for Disease Control and Prevention (CDC) was undercounting the serious adverse event rate by a factor of 40, that vaccine injury is real, the vaccine-injured need to be taken seriously and treated, and that doctors need to be able to voice their opinions openly without fear of retribution so treatments for the vaccine-injured can be developed.
9. In this interview, Matthes is asked about Andreas Schöfbeck, the insurance company executive who was fired after raising concerns about vaccine injury based on claims data:“He should have said there is a clue here, but causality has yet to be verified. It wasn’t entirely clear if he was speaking politically, or if he was just doing his due diligence and saying: Here’s a signal that needs to be investigated further, please. That little differentiation cost him his job.
“But if you then look at how black and white is currently being painted in public and with what vehemence certain opinions are exchanged without there being any facts — then you realize how unfairly he was punished for something that maybe was not quite carefully worded.”
You can tell Matthes is being very cautious in his choice of words, but one can hardly justify Schöfbeck’s firing on the grounds that he was not guarded enough in his statements. (I’d bet dollars to donuts he would have been fired even if his statement was more carefully worded.)
10. Curiously, Matthes says the eight per 1,000 serious event rate “corresponds to what is known from other countries such as Sweden, Israel or Canada. Incidentally, even the manufacturers of the vaccines had already determined similar values in their studies.”
Is this true? My experience from Israel says it’s not. Perhaps there is some wiggle room, as according to this article, the study defines “serious events” as “symptoms that require medical treatment and last for several weeks or months.”
As far as I know, no study or data out of Israel has tracked serious events by that definition. If anybody knows what data he is comparing to, in Israel or elsewhere, please let us know in the comments.
11. Of course there are a lot of possible biases in the survey methodology. Unfortunately, I was not able to find any details on the methodology of the survey, so a more complete discussion of that will have to wait for another time.
One thing for sure: People who died from the vaccine can’t answer a survey, so the research has nothing to say on this issue.
Here are links to some of the articles I found on this story in the mainstream German press: 1, 2, 3, 4. Machine translation is more than serviceable.
And here is a video (again in German) from a mainstream German broadcaster on vaccine injuries, including an interview with Matthes. No translation is possible.
Originally published on Josh Guetzkow’s Jackanapes Junction Substack page.

![]() by Belligerent Savant » Sun May 22, 2022 1:20 pm
by Belligerent Savant » Sun May 22, 2022 1:20 pm
Is Subject #12312982 the Key to Proving Pfizer Vaccine Trial Fraud?
The Story of Augusto Roux
Subject # 12312982 in Pfizer study C4591001 is Augusto Roux, a 35-year old lawyer from Buenos Aires, Argentina who volunteered for Pfizer’s stage 3 trial of its COVID-19 vaccine (or whatever you want to call it) in order to protect his mother with emphysema.
His story and some of the shenanigans surrounding the Argentinian trial site have been amply covered by Dr. David Healy in three sprawling but extremely important blog posts: 1, 2, 3. The first one was published March 1st, but it was only last week that I caught on to this story, so I’m assuming most of you probably aren’t familiar with it. So please share this — we’ve got to get the word out, because Augusto Roux may very well hold the key to bringing down the Pfizer vaccine trial, or a least proving fraud at the largest trial site that was home to over 10% of the participants in the trial.
If you don’t have time to sink your teeth into David’s posts (even just the 1st one), I’ll bring you up to speed on key details:
On the way home after his second dose on Sept. 9, 2020, he began feeling unwell, developed a high fever and felt terribly ill until he fainted on Sept. 11 and finally went to the hospital on Sept. 12 (not the one where the trial was being run). They did a thorough work-up, including a CAT scan of his chest that showed an abnormal collection of fluid around the outside of the heart. Basically he had pericarditis.
On Sept. 14, he was discharged. The doctor wrote in his chart that he had suffered an adverse reaction to the vaccine. Augusto was told by hospital staff they there had been a huge influx of people from the clinical trial coming to the hospital (there were 2,981 subjects enrolled in the trial before Augusto), so his experience was not new to them. (The trial site managed to enlist several thousand subjects in just a few weeks.) One nurse estimated they had seen around 300 people.
Now here’s where it gets really interesting, and we know all of this because Augusto, a lawyer, successfully sued to get his medical and trial clinical records, even though it took him over a year. I will try to make a long story short:
Even though Augusto had a negative PCR test at the hospital, and even though the doctor at the hospital wrote that his condition was due to the vaccine, when Augusto called the trial site on Sept. 14 to notify them he was in the hospital, they wrote down in his clinical trial record that he had been admitted for a bilateral pneumonia that had nothing to do with the “investigational product” — even though that was not what he told them.
On October 7, the clinical trial notes that “at the request of the sponsor” (AKA Pfizer), the adverse event code was update to COVID-19 disease. And that’s how Pfizer made cases of myocarditis and pericarditis disappear, by sweeping them under the rug of COVID-19. Moreover, the diagnosis of COVID-19 would not count against the efficacy calculations, since those required a positive PCR test to confirm diagnosis.
Two days later On Oct. 9, Augusto was formally unblinded. The principal investigator for the trial, Fernando Polack, had told him that Augusto could only be unblinded if his life were in danger, which is simply untrue. So Augusto appealed to ANMAT, the Argentinian FDA. In a formal hearing they forced the trial investigators to tell Augusto if he had received the vaccine or not. He had. If you think the timing of the Oct. 7 request by Pfizer to change his AE is suspect, you’re not alone.
A day before the hearing (and a day after the change in AE status), Polack wrote in Augusto’s clinical trial records that he had had an attack of severe anxiety starting on September 23, not caused by the vaccine, and wrote that Augusto suspected a conspiracy between the two hospitals, described his anxiety as constitutional, and noted that it was ongoing.
To add insult to injury, two days after the ANMAT hearing, Polack had the mental health diagnosis added to Augusto’s actual medical records. Of course a pediatrician like Polack has no business making mental health diagnoses, especially without any formal assessment.
Recall that Polack was the first author on the December, 2020 NEJM paper on the safety and efficacy of the vaccine. He is also one of the directors of i-trials, the site management organization paid handsomely by Pfizer to run the trial in Argentina (the largest site of the trial by far). If he raised an alarm about the vaccine safety, his company would have lost a ton of money and would be an unlikely choice by any company to run any trials in the future. So to say that he had an interest in achieving a positive trial outcome would be quite an understatement. There may be other conflicts we’re not aware of.
I spoke with Augusto at length over zoom last week. Such a nice man. He told me he has recordings of Polack and another senior trial investigator admitting to him over the phone in separate conversations that somebody at the trial site died. However, according to information provided to a member of the Argentine parliament, nobody is recorded as having died in the trial at that site. We still have to confirm that, but if true it’s huge. He has other information about severe adverse events that were covered up by the trial investigators. But his well-document case alone is enough to sink the ship.
Now, the last set of files released as part of the FDA FOIA document dump included several data files from the trial, including a dataset with all of the protocol deviations recorded during the trial. These occur whenever the study protocol is not followed, and they are supposed to be recorded.
So what do these records indicate for Augusto? Here are the 3 deviations listed:2020-09-12 Nasal swab not collected for the visit where it is required
2020-09-12 Visit performed outside of protocol specified window.
2020-10-09 Blind compromised
We know that Augusto did not visit the trial site on Sept. 12 because he was in the hospital. Apparently the “visit performed” they refer to is his hospitalization. And while it is technically true that the trial site did not collect the swab for the PCR, a swab was collected and a test done, just not at the trial site. And it correctly records his blind as having been compromised on Oct. 9. But, oddly, in the field reserved to record the ‘unblinding date,’ none is given. Furthermore, even though the unblinding should have been grounds to exclude Augusto from the trial efficacy analyses, it was not marked as important or as something worthy of exclusion.
There are many fishy things in the protocol deviation data, which I will be writing about soon. So, as they say, watch this space!
@JeanRees10
Highly recommend a read about Augusto Roux, who was in the Pfizer Clinical Trial, in Argentina.
@DrDavidHealy
documents his story with medical records, a timeline, as well as illustrative descriptions
Augusto, too, had an anxiety note/dx - October 11th
https://davidhealy.org/disappeared-in-argentina/
@ITGuy1959
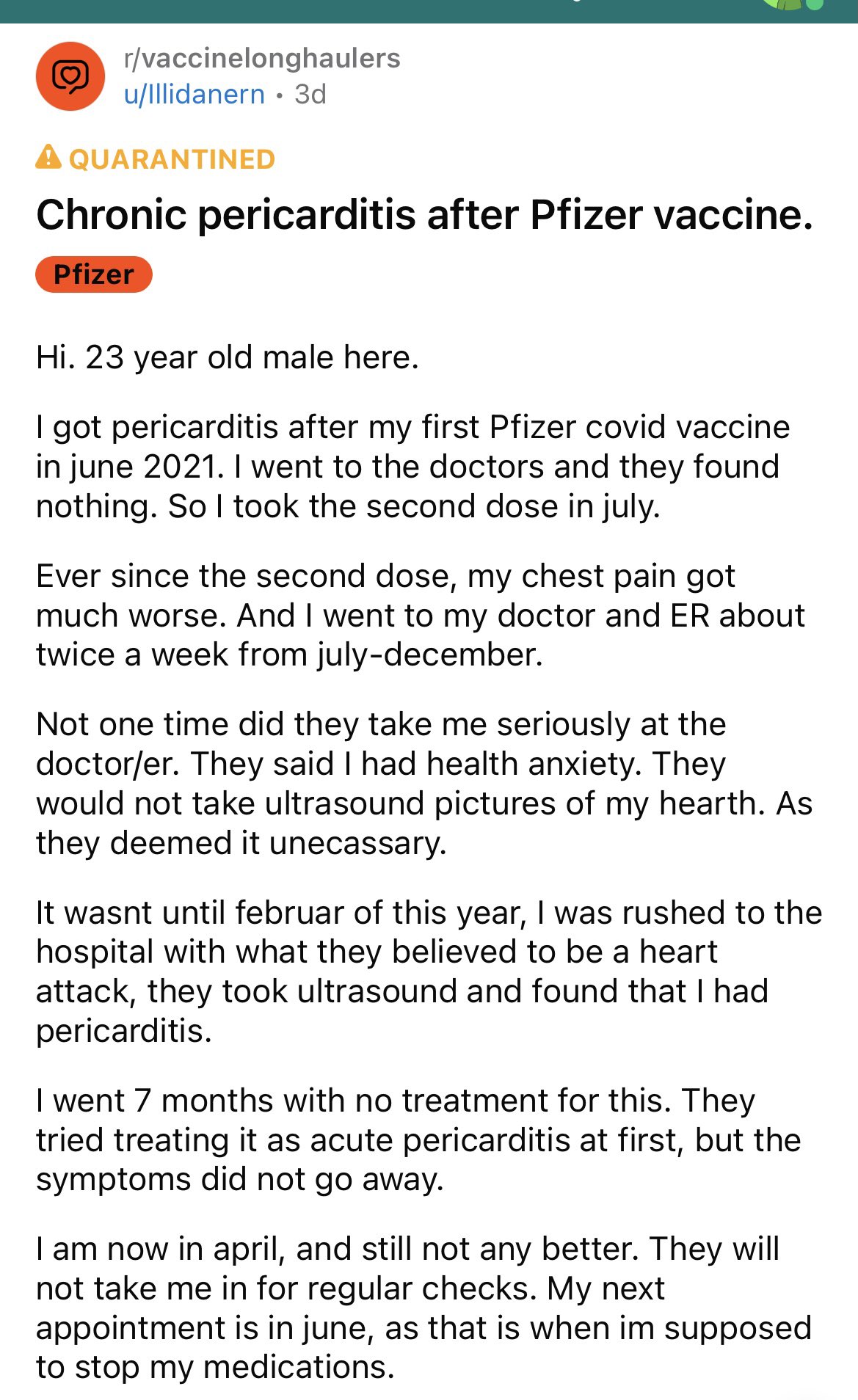
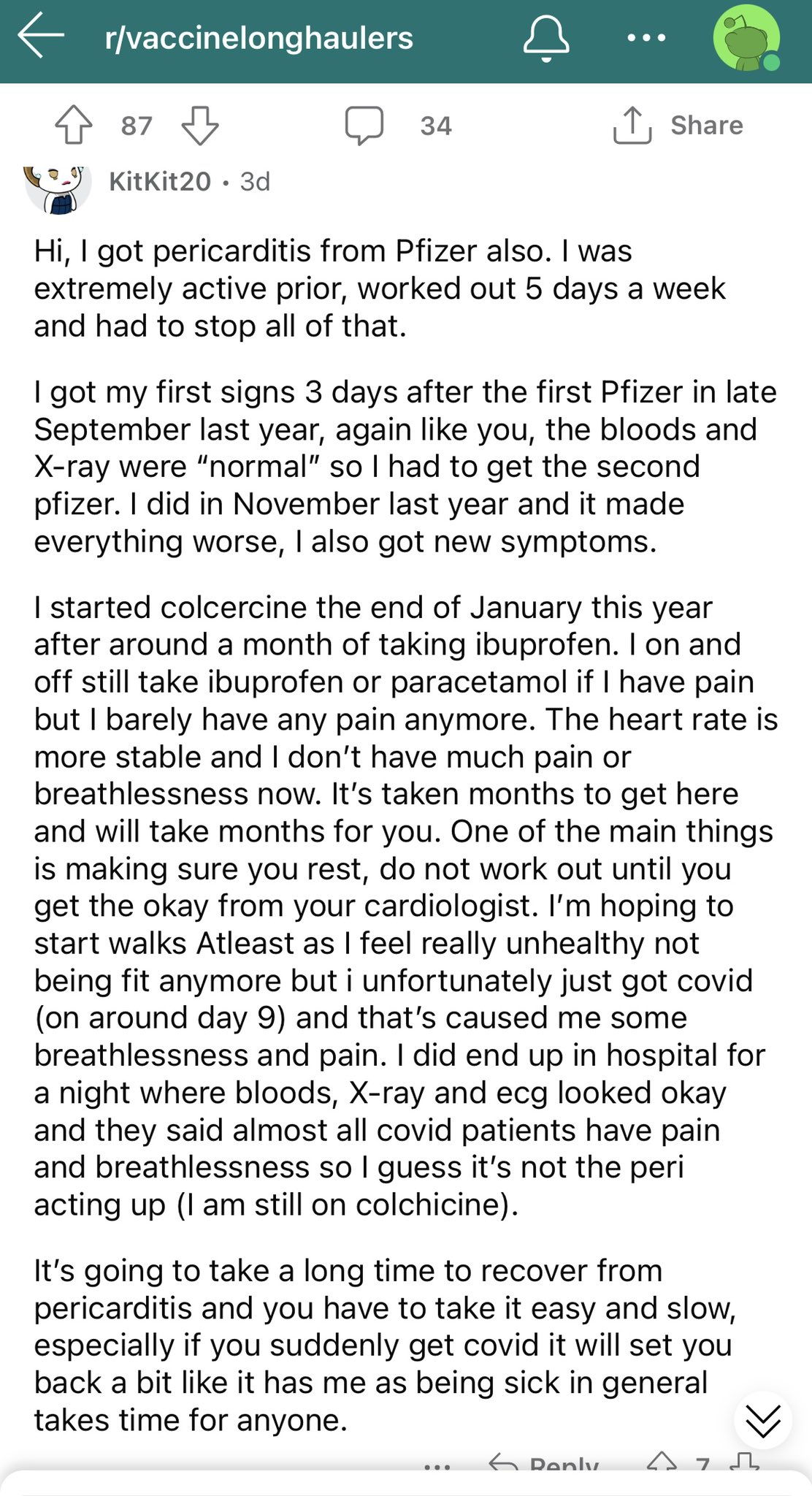
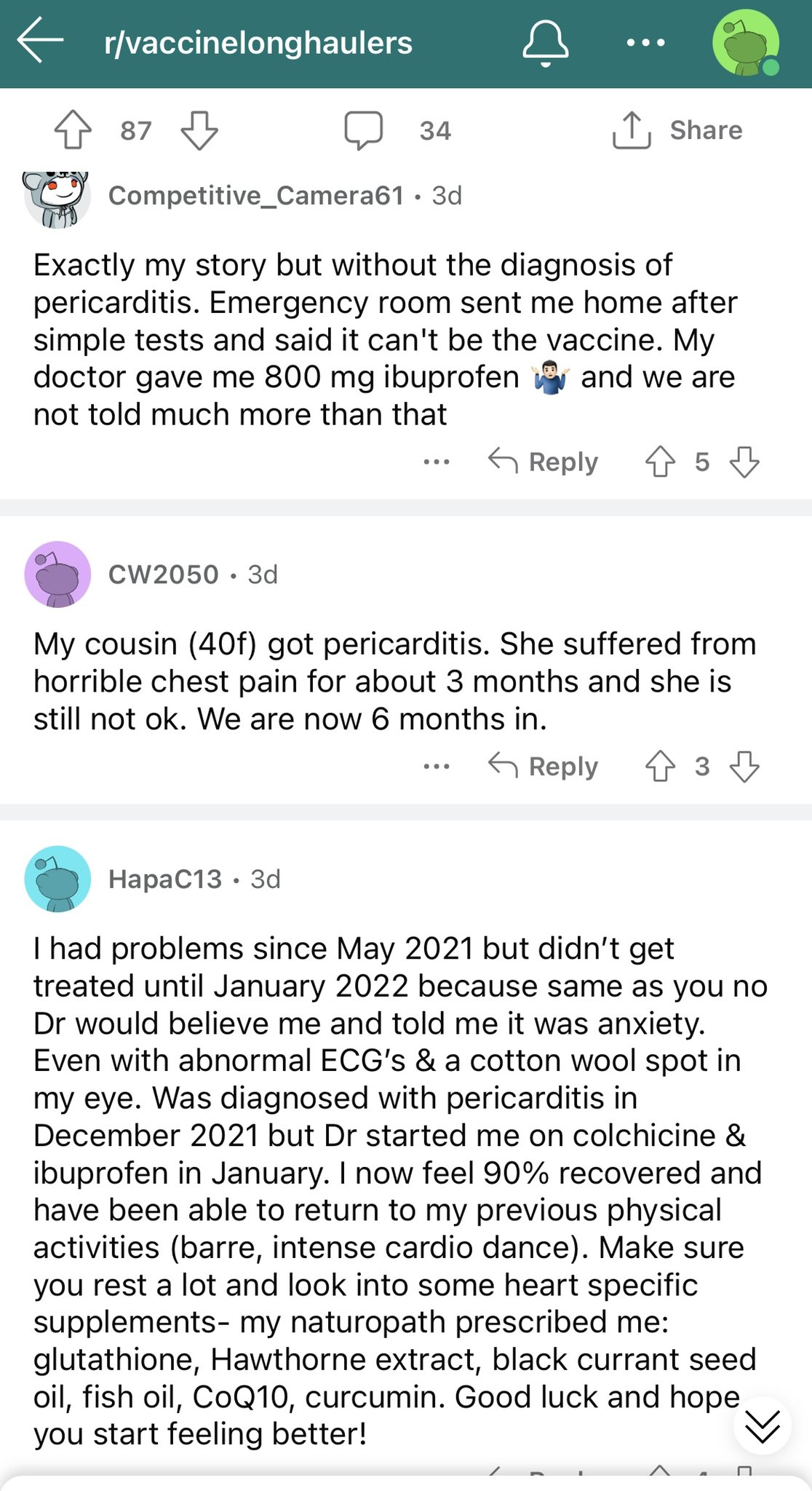
Meanwhile over on Reddit this is awful. As if pericarditis isn’t bad enough, imagine getting written off time and again as “anxiety”.
There were many more “Me too” replies than room to post.
(Sometimes) safe and effective.

![]() by Belligerent Savant » Mon May 23, 2022 8:42 pm
by Belligerent Savant » Mon May 23, 2022 8:42 pm
Mark Changizi
@MarkChangizi
“Recent observations from surveillance data [suggests] that N antibody levels appear to be lower in individuals who acquire infection following 2 doses of vaccination.”
- Page 23, UK Health Security Agency COVID-19 Vaccine Surveillance Report,
Week 42”
https://assets.publishing.service.gov.u ... eek-42.pdf
![]() by Belligerent Savant » Sat Jun 04, 2022 2:43 pm
by Belligerent Savant » Sat Jun 04, 2022 2:43 pm
@jstylman
·
Jun 3
I've been a sports fan all my life and don't recall young, elite athletes suffering from heart issues, strokes & dying suddenly. Someone put together this list which doesn't even cover the breadth of this issue.
Seems worthy of a public discussion, no?
https://airtable.com/shrbaT4x8LG8EbvVG/ ... SUIOPAa7Mx
2021 - 2022 Epidemic of Heart Issues in Athletes - Chronological Order
![]() by DrEvil » Sun Jun 05, 2022 2:23 pm
by DrEvil » Sun Jun 05, 2022 2:23 pm

![]() by Belligerent Savant » Sun Jun 05, 2022 2:33 pm
by Belligerent Savant » Sun Jun 05, 2022 2:33 pm
Belligerent Savant » Tue Nov 30, 2021 12:05 am wrote:.
https://boriquagato.substack.com/p/is-i ... ource=copyis it vaccines or is it covid causing athletes to collapse on the field?
a little crowd sourced homework project.
it has become manifestly clear that we’re seeing an extreme outcome in athletes and heart conditions. something is very much amiss.
there is quite a lot of evidence that this seems to be a vaccine effect (https://boriquagato.substack.com/p/athl ... s-and-life). but, predictably, the chorus from team mask up, lock down, and vax, vax, vax, vax, vax is taking the other side of this argument and claiming it’s covid.
predictably, there is not a shred of supporting data, just supposition and appeals to ever more tatterdemalion authority.
there are a number of reasons that i find this argument uncompelling, but there is an aspect of it that i find quite revelatory as well:
they have stopped denying that it’s happening.
it has become sufficiently common and sufficiently obvious that they can no longer ignore it and must address it instead and offer up an explanation.
as i will lay out below, this poses a serious problem for them because now we have a testable hypothesis.
if we agree that athletes are, indeed having an extremely disproportionate number of heart issues of late, then the “why” can be assessed by timing.
- if it’s covid causing this issue, it should have been present last year as well.
- if it’s the vaccines, this issue should have emerged in 2021 but not in 2020.
we have a strong base prior for this effect from these vaccines. they have been shown to accumulate in heart tissue and to elicit a FAR stronger antibody response than just having had covid. this is due to the larger dose of S-1 protein. (it also appears to confer no clinical benefit whatsoever as natural recovery is far more potent and more sterilizing than vaxxed)
so, it’s quite reasonable to presume more heart risk. there has been almost none in the young from covid. 2020 a 2019. but look what happened in 2021 after vaccination.
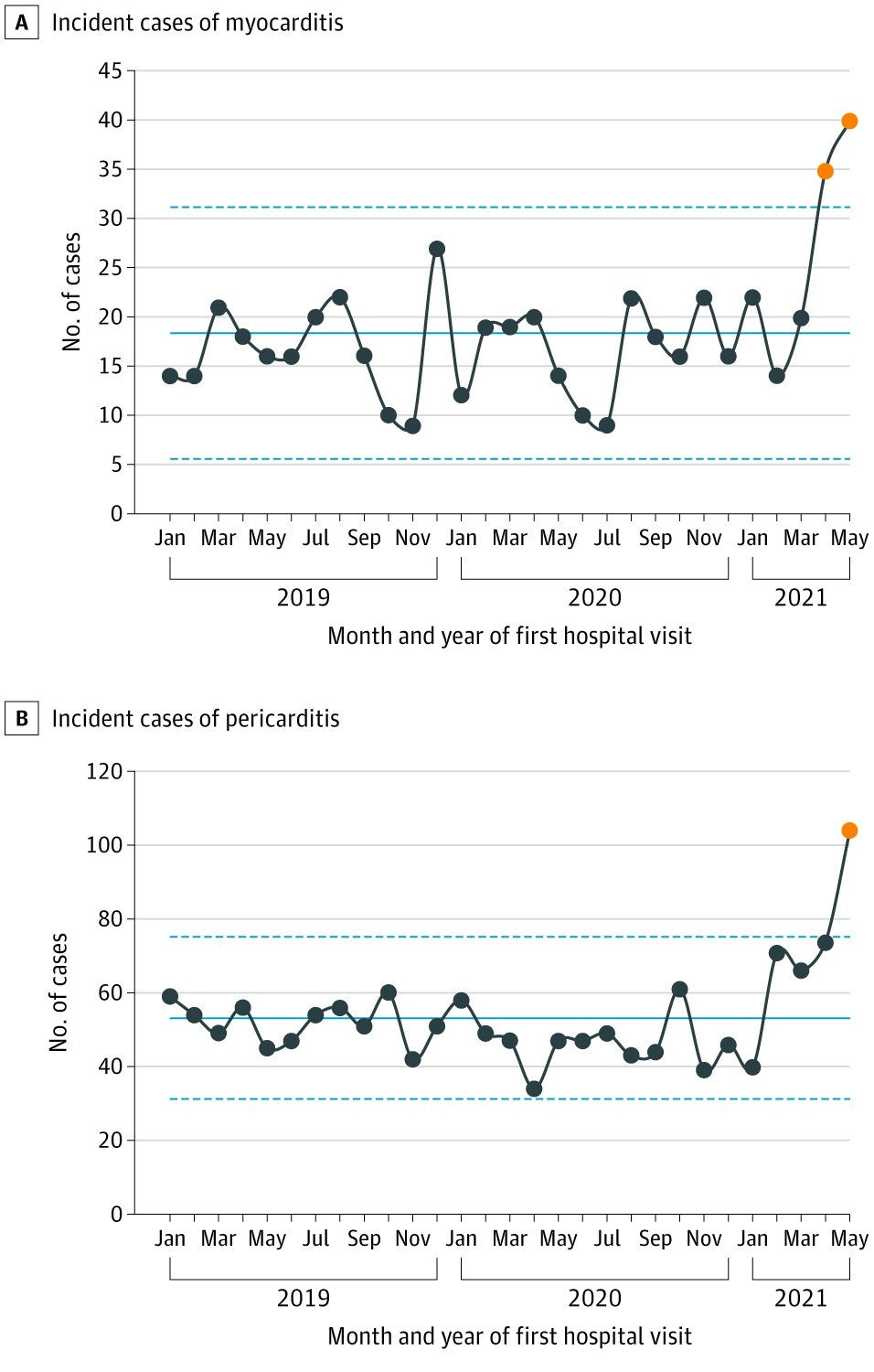
https://jamanetwork.com/journals/jama/f ... le/2782900
this is very much the opposite of what one would expect were this caused by covid but exactly what one would expect if it were caused by vaccine.
and a lot of people are starting to notice.
numerous EU countries have discontinued used of these mRNA vaccines in the young over adverse events risk (particularly heart risk) swamping benefit.
and the data on this keeps getting worse. (though any such reporting in the US is conspicuously absent)@FZores
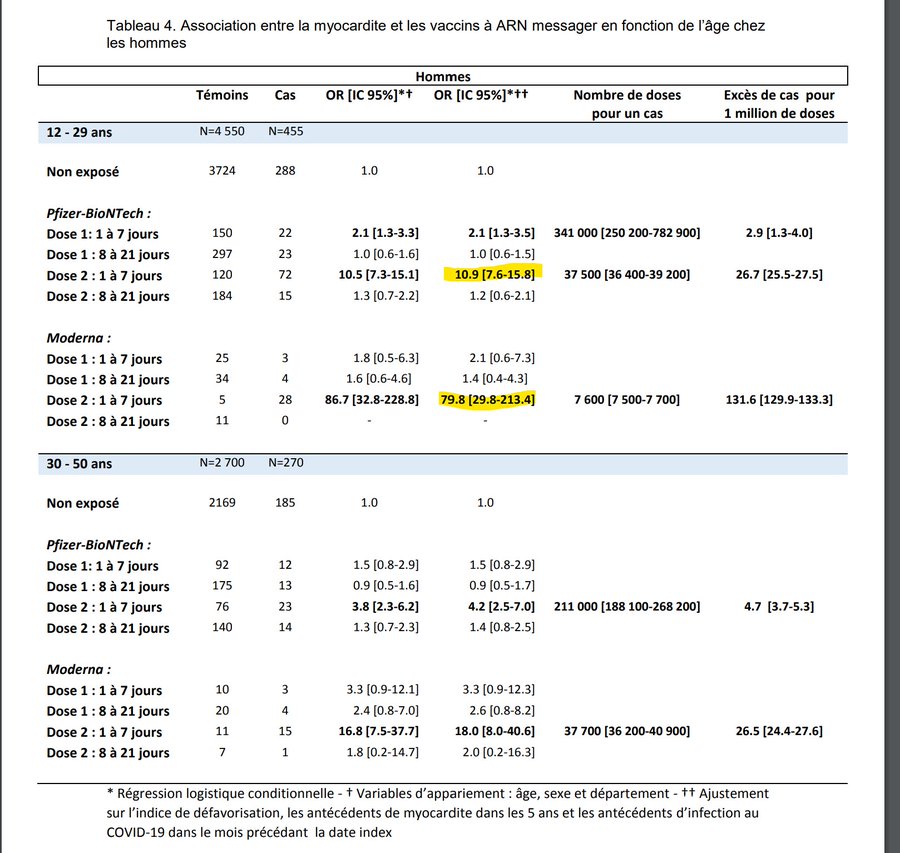
For men under 30
2nd dose of pfizer vaccine associated with an OR of hospitalization for myocarditis of 10,9.
1 hospitalization for 37.500 shots
2nd dose of moderna vaccine associated with an OR of hospitalization for myocarditis of 79.
1 hospitalization for 7.600 shots
unfortunately, a lot of people, especially in the US, are determined to suppress such findings. “hey, those vaccines we approved without sound trials, won’t give you the data on, mandated and hectored over, and pushed on your kids while absolving the pharma companies from any liability whatsoever, yeah, sorry, it was really unsafe” is not a great look.@GBNEWS
'They aren't going to publish their findings, they are concerned about losing research money'
Dr Aseem Malhotra reveals a cardiology researcher found similar results to a new report showing an increase in risk of heart attack following the mRNA COVID vaccine.
this sort of suppression is literally the opposite of public health. how can people make sound choices in the absence of sound data?
so here’s a little crowd sourced homework assignment:
i recall basically no athletes collapsing from heart issues in 2020. this looks to me to have started in the spring of 2021 when vaccinations ramped up.
but it’s possible i’m wrong or suffering from confirmation bias in perception. it looks like a validated rise, but perhaps it’s not.
so let’s validate or refute it. see what you can find. let’s compile something like a list, see how good a data set can be assembled, and see what the data looks like.
this is the sort of capability the modern info-sphere provides us with.
if “authorities” will not collect good data, then let’s collect our own.
![]() by Joe Hillshoist » Mon Jun 06, 2022 1:15 am
by Joe Hillshoist » Mon Jun 06, 2022 1:15 am
DrEvil » 06 Jun 2022 04:23 wrote:If I remember correctly, on average 2-3 athletes drop dead every week, and that's without covid or vaccines in the picture. We just never heard about it before because nobody outside the local press used to care if some junior league football player from Nigeria dropped dead. Now that people are collating all the deaths it suddenly looks like a lot.
Not saying there's nothing there, but athletes used to drop dead all the time before covid too, so without a comparison of before and after numbers it doesn't really say much. Would also be interesting to know how many of them had covid at some point before dropping dead.
![]() by Joe Hillshoist » Mon Jun 06, 2022 1:16 am
by Joe Hillshoist » Mon Jun 06, 2022 1:16 am
![]() by Joe Hillshoist » Mon Jun 06, 2022 1:19 am
by Joe Hillshoist » Mon Jun 06, 2022 1:19 am
Belligerent Savant » 06 Jun 2022 04:33 wrote:But in my view (shared by a growing count of others) there is little doubt these shots are far more likely to cause near-term damage to the young than the virus itself.
![]() by drstrangelove » Mon Jun 06, 2022 8:03 pm
by drstrangelove » Mon Jun 06, 2022 8:03 pm
Joe Hillshoist » Mon Jun 06, 2022 1:15 am wrote:DrEvil » 06 Jun 2022 04:23 wrote:If I remember correctly, on average 2-3 athletes drop dead every week, and that's without covid or vaccines in the picture. We just never heard about it before because nobody outside the local press used to care if some junior league football player from Nigeria dropped dead. Now that people are collating all the deaths it suddenly looks like a lot.
Not saying there's nothing there, but athletes used to drop dead all the time before covid too, so without a comparison of before and after numbers it doesn't really say much. Would also be interesting to know how many of them had covid at some point before dropping dead.
This is true. Even issues like tachycardia are more common in elite athletes because of training loads and working wioth a HR around 200 bpm.
But at the same time if there is a problem it will manifest in elite sporting competitions.
There are about 1000 AFL players or players trying to make that league in Australia. They've all been vaccinated.
One is mentioned in that link about the epidemic of heart issues. Jake Lever. plays for the Melbourne Demons. He's one of the best players at his position in the comp and is tearing it up again.
Dr Strangelove mentioned another - Ollie Wines. He won the Brownlow medal last year for the comp's best and fairest. Wines had heart issues - an irregularity - but rejected the idea that they were caused by vaccines, to the point where he issued a straight up denial. He's back playing and dominating as he was previously.
One player did have a vaccine related injury. Jed Anderson. Plays for the club I've supported all my life and am a member of and is one of my favorite players. He was diagnosed with pericarditis after his first dose of an (Unknown) mRNA vaccine. Vaccines were mandated and Jed basically said he wasn't playing this year if he had to have another mRNA shot. He's on about half a million dollars a year, but is an indigenous guy from the NT who prefers living in the bush. He was happy to stay there. Eventually the Novavax vaccine became available and after he'd recovered from pericarditis he took that and is now back playing as well and has been our best player over the last two rounds (imo anyway. We're struggling tho this season.)
AFL is probably the hardest team sport in terms of endurance and cardio fitness requirements. Wines and Jedly are both midfielders and will run between 12 and 15 kms in a game. Games go for 4 x 20 minute quarters that end up lasting 30-35 minutes with stoppages and players are on the move for nearly all of that 35 minutes, competing hard and with alot of wrestling and physical contact.
Jed was the only player with a vaccine injury in the comp. Its taken him three months to get back to full fitness. No way you could perform to the level required with a vaccine injury. You would have a heart attack or other issue on field. Well actually you'd cop it during pre season cos the training loads are massive. It would be impossible to hide.
There are 18 sides in the comp with lists of up to 44 players. There would be another 200 around the country in the state leagues who would think they were a chance at breaking into the comp and every year up to 1000 kids nominate to be drafted into those 18 sides, with up to 100 being taken. Every one of those people have to be vaccinated now. I don't think boosters are mandatory tho. Plenty of players have had covid now as well.
AS far as I know, and I'm trying to follow it (tho kids medical status isn't something I can find out easily and it none of my business really), no one else has had a vaccine injury. There may be some question over Jake Lever but he missed no training or footy. So its highly unlikely he had a heart issue.
Despite the original claims of much lower rates the actual rate of vaccine injury is at least 1 in 1500 in terms or peri or myocarditis. At least for young men - the most vulnerable group for vaccine injuries to the heart. This has been shown by plenty of independent research and from insurance company figures after the vaccination program was well under way.
Jed's injury, the only one in the AFL so far, fits that rate and is defintiely confirmation that the original side effect rates pfizer et al were claiming are bullshit.
People die playing footy in Australia every year and have for as long as I can remember. i was still p[laying in my 40s and even tho i was pretty fit back then smoked weed and tobacco. Not at the highest level obviously. I'd always have people telling me to retire cos of the risk of heart attack. Once I got over 35, about the time I joined this board, they started talking about it, but it was only dodgy knees and hamstrings that eventually stopped me.

![]() by Belligerent Savant » Tue Jun 07, 2022 2:32 pm
by Belligerent Savant » Tue Jun 07, 2022 2:32 pm
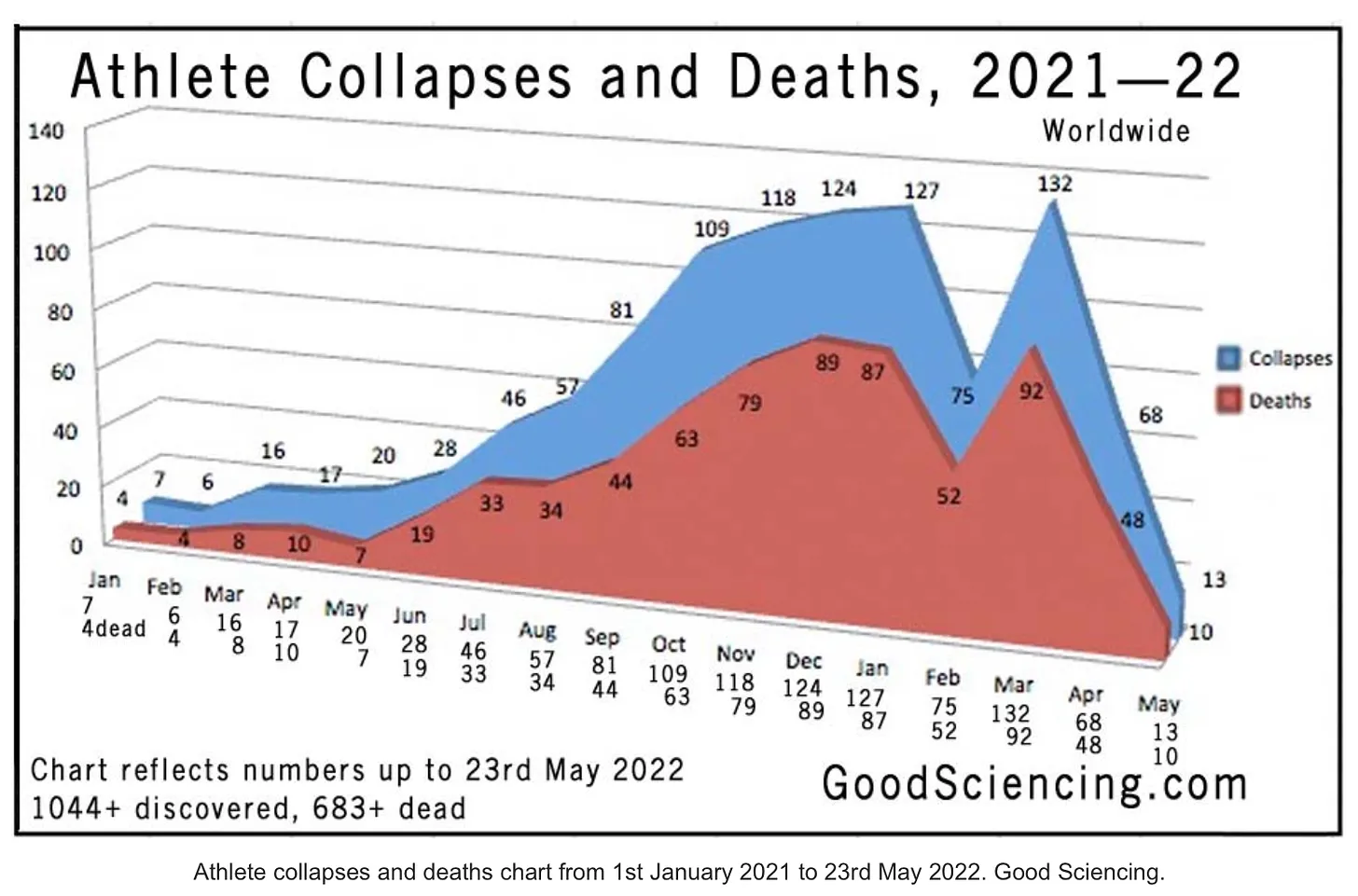
A 2006 journal article titled “Sudden cardiac death in athletes: the Lausanne Recommendations,” provides data on historic athlete cardiac deaths. The study discloses that, over a 35-year period between 1966-2004, “sudden cardiac death” occurred in 1,101 reported cases in athletes under 35 years old, or an average of about 31 per year, or 2.5 deaths per month.
Another study on cardiac disease in US athletes, over a 26 year period between 1980 to 2006 in thirty-eight sports, found 1,866 deaths of athletes with cardiac disease — about 71 deaths per year on average, or 5.9 per month.
In 2021, 394 athlete deaths were reported, plus 279 for the 2022 year to date. That’s an average of 42 per month between 2021-2022. So, in other words, it’s not just your imagination.
University of Massachusetts Amherst lacrosse player Aidan Kaminska, 19, died “unexpectedly” on May 30, according to an online obituary. No cause of death provided.
Jayda Grant, 20, track athlete and daughter of Dayton basketball coach Anthony Grant, died suddenly and unexpectedly Friday. The Greene County Coroner’s Office told a WHIO-TV reporter that her death was “still under investigation.”
The loss of these young lives is a tragedy. I hope that one day the families will receive closure and transparency.
Sudden cardiac death in athletes: the Lausanne Recommendations
2006 Dec
Karin Bille 1, David Figueiras, Patrick Schamasch, Lukas Kappenberger, Joel I Brenner, Folkert J Meijboom, Erik J Meijboom
Affiliations expand
Abstract
Objectives: This study reports on sudden cardiac death (SCD) in sport in the literature and aims at achieving a generally acceptable preparticipation screening protocol (PPSP) endorsed by the consensus meeting of the International Olympic Committee (IOC).
Background: The sudden death of athletes under 35 years engaged in competitive sports is a well-known occurrence; the incidence is higher in athletes (approximately 2/100,000 per year) than in non-athletes (2.5 : 1), and the cause is cardiovascular in over 90%.
Methods: A systematic review of the literature identified causes of SCD, sex, age, underlying cardiac disease and the type of sport and PPSP in use. Methods necessary to detect pre-existing cardiac abnormalities are discussed to formulate a PPSP for the Medical Commission of the IOC.
Results: SCD occurred in 1101 (1966-2004) reported cases in athletes under 35 years, 50% had congenital anatomical heart disease and cardiomyopathies and 10% had early-onset atherosclerotic heart disease. Forty percent occurred in athletes under 18 years, 33% under 16 years; the female/male ratio was 1/9. SCD was reported in almost all sports; most frequently involved were soccer (30%), basketball (25%) and running (15%). The PPSP were of varying quality and content. The IOC consensus meeting accepted the proposed Lausanne Recommendations based on this research and expert opinions (http://multimedia.olympic.org/pdf/en_report_886.pdf).
Conclusion: SCD occurs more frequently in young athletes, even those under the age of 18 years, than expected and is predominantly caused by pre-existing congenital cardiac abnormalities. Premature atherosclerotic disease forms another important cause in these young adults. A generally acceptable PPSP has been achieved by the IOC's acceptance of the Lausanne Recommendations.
...
The 1101 cases were grouped after pathology, according to the cardiovascular diagnosis, into 10 groups and 31 subgroups, as shown in Table 4. Coronary artery anomalies, half of them being anomalies of the origin of the coronary artery, the other half anomalies of the course of the coronary artery, and hypertrophic cardiomyopathy (HCM) are the two largest groups, with 262 and 261 cases, respectively. Traumatic cases of SCD being excluded (103 cases), there are 998 remaining cases, as shown in Fig. 1.
I have a question about this: the athlete deaths increased 42/2.5 which is >16X.
Why don't we see the same increase in general population? Or at least in young healthy people? The worst estimate I have seen is 2X increase for young people.
Hypothesis:
- Athletes are pushing themselves to the limit so any damage will be obvious. If that's the case, the damage is there so we should expect life expectancy to be reduced by decades for foxed people. What's the average age of death for people with chronic health issues?
Could there be something else going on, but what? I don't buy the "it's the climate change, or the applause, or..." Anybody has any idea?
Reply:
Physically and immunologically, serious athletes are very fragile. They are also bad at listening to their bodies and allowing themselves sufficient recovery time so that tends to ingrain damage. They also tend to have high levels of inflammation going on all the time. I imagine those things make them especially vulnerable to foxes, just like a diabetic.
![]() by Joe Hillshoist » Wed Jun 08, 2022 7:50 pm
by Joe Hillshoist » Wed Jun 08, 2022 7:50 pm
drstrangelove » 07 Jun 2022 10:03 wrote:Joe Hillshoist » Mon Jun 06, 2022 1:15 am wrote:DrEvil » 06 Jun 2022 04:23 wrote:If I remember correctly, on average 2-3 athletes drop dead every week, and that's without covid or vaccines in the picture. We just never heard about it before because nobody outside the local press used to care if some junior league football player from Nigeria dropped dead. Now that people are collating all the deaths it suddenly looks like a lot.
Not saying there's nothing there, but athletes used to drop dead all the time before covid too, so without a comparison of before and after numbers it doesn't really say much. Would also be interesting to know how many of them had covid at some point before dropping dead.
This is true. Even issues like tachycardia are more common in elite athletes because of training loads and working wioth a HR around 200 bpm.
But at the same time if there is a problem it will manifest in elite sporting competitions.
There are about 1000 AFL players or players trying to make that league in Australia. They've all been vaccinated.
One is mentioned in that link about the epidemic of heart issues. Jake Lever. plays for the Melbourne Demons. He's one of the best players at his position in the comp and is tearing it up again.
Dr Strangelove mentioned another - Ollie Wines. He won the Brownlow medal last year for the comp's best and fairest. Wines had heart issues - an irregularity - but rejected the idea that they were caused by vaccines, to the point where he issued a straight up denial. He's back playing and dominating as he was previously.
One player did have a vaccine related injury. Jed Anderson. Plays for the club I've supported all my life and am a member of and is one of my favorite players. He was diagnosed with pericarditis after his first dose of an (Unknown) mRNA vaccine. Vaccines were mandated and Jed basically said he wasn't playing this year if he had to have another mRNA shot. He's on about half a million dollars a year, but is an indigenous guy from the NT who prefers living in the bush. He was happy to stay there. Eventually the Novavax vaccine became available and after he'd recovered from pericarditis he took that and is now back playing as well and has been our best player over the last two rounds (imo anyway. We're struggling tho this season.)
AFL is probably the hardest team sport in terms of endurance and cardio fitness requirements. Wines and Jedly are both midfielders and will run between 12 and 15 kms in a game. Games go for 4 x 20 minute quarters that end up lasting 30-35 minutes with stoppages and players are on the move for nearly all of that 35 minutes, competing hard and with alot of wrestling and physical contact.
Jed was the only player with a vaccine injury in the comp. Its taken him three months to get back to full fitness. No way you could perform to the level required with a vaccine injury. You would have a heart attack or other issue on field. Well actually you'd cop it during pre season cos the training loads are massive. It would be impossible to hide.
There are 18 sides in the comp with lists of up to 44 players. There would be another 200 around the country in the state leagues who would think they were a chance at breaking into the comp and every year up to 1000 kids nominate to be drafted into those 18 sides, with up to 100 being taken. Every one of those people have to be vaccinated now. I don't think boosters are mandatory tho. Plenty of players have had covid now as well.
AS far as I know, and I'm trying to follow it (tho kids medical status isn't something I can find out easily and it none of my business really), no one else has had a vaccine injury. There may be some question over Jake Lever but he missed no training or footy. So its highly unlikely he had a heart issue.
Despite the original claims of much lower rates the actual rate of vaccine injury is at least 1 in 1500 in terms or peri or myocarditis. At least for young men - the most vulnerable group for vaccine injuries to the heart. This has been shown by plenty of independent research and from insurance company figures after the vaccination program was well under way.
Jed's injury, the only one in the AFL so far, fits that rate and is defintiely confirmation that the original side effect rates pfizer et al were claiming are bullshit.
People die playing footy in Australia every year and have for as long as I can remember. i was still p[laying in my 40s and even tho i was pretty fit back then smoked weed and tobacco. Not at the highest level obviously. I'd always have people telling me to retire cos of the risk of heart attack. Once I got over 35, about the time I joined this board, they started talking about it, but it was only dodgy knees and hamstrings that eventually stopped me.
The one thing I'm curious about is the portion of players who received astrazeneca and then got novavax for the booster. I kind of suspect that is a significant portion of them.
As to the boosters, there was a loop hole if you tested positive. Which means if players got together behind the scenes and said no, the club could just get the med team to keep PCR testing them until they return a false positive.
![]() by drstrangelove » Sun Jun 12, 2022 4:12 am
by drstrangelove » Sun Jun 12, 2022 4:12 am
FDA says Moderna vaccine for youngest children is safe and effective
Scientists at the Food and Drug Administration on Friday said Moderna’s coronavirus vaccine for infants and young children was safe and effective, setting the stage for a review by the agency’s outside advisers Wednesday and a potential authorization by the end of the week.
The analysis was released in briefing documents ahead of next week’s meeting, when the independent advisers also will consider whether a vaccine by Pfizer and its German partner, BioNTech, should be authorized for the youngest children. Babies and children younger than 5 — a group numbering 19 million — remain the only age group in the United States still not eligible for a coronavirus vaccine.
Moderna has asked the FDA for permission to use its vaccine in children 6 months through 5 years old. The Pfizer-BioNTech request is for children 6 months through 4 years old. The FDA is expected to release its assessment of the Pfizer-BioNTech vaccine in the next few days.
The FDA said the Moderna two-shot regimen for the youngest children met the main requirement set by regulators — that it generate an immune response at least as strong as the protection afforded young adults. The vaccine, according to data from the company and confirmed by the FDA, was only somewhat effective in preventing illness among the youngest group of recipients, reflecting the impact of the highly transmissible omicron variant, which has blunted the power of the vaccine in adults as well.
In examining side effects, the agency said adverse reactions in younger children were generally lower compared with those observed in adolescents and young adults, except for fevers. The FDA said the rates of fevers after vaccination were not “substantially different” than for other childhood vaccines.
In addition to the youngest children, Moderna is seeking authorization for its vaccine for children 6 to 17 years old. The agency gave a similarly favorable evaluation for those ages. The company’s request for the older children and teenagers will be reviewed Tuesday by the advisory committee.
Only Pfizer-BioNTech shots are authorized for Americans under 18.
The FDA said that, taken together, the Moderna data on safety, immune response and effectiveness indicates the pediatric vaccine has “a favorable benefit-risk profile in all age groups evaluated.”
While youngsters don’t usually become seriously ill with covid-19, more than 1,200 children and adolescents have died in the United States since the beginning of the pandemic in early 2020. And hospitalizations increased during the wave spawned by the omicron variant of the coronavirus.
If all goes as expected — the FDA is not required to follow the recommendations of its outside experts, but often does — the agency will authorize the Moderna and Pfizer-BioNTech vaccines for the youngest children soon after the advisory committee meeting. Assuming the Centers for Disease Control and Prevention and its advisers recommend the shots, the vaccines will be available in pediatricians’ offices, hospitals, clinics and certain pharmacies beginning the following week.
The Biden administration has been foreshadowing the regulatory action for days, pledging to speed supplies to an array of distribution sites. White House health officials said Thursday they are working closely with community and medical groups to ensure families have answers to questions about the vaccines.
Moderna’s two doses for the youngest group are each 25 micrograms, one-quarter of the adult dose, administered four weeks apart. The vaccine was shown to be 51 percent effective in preventing illness in children between 6 months and 2 years old, and 37 percent effective in children 2 to 5 years old. The FDA said it expects the vaccine will provide stronger protection against severe disease and hospitalizations.
The Pfizer-BioNTech vaccine is three shots, with the second dose given three weeks after the first. The third shot typically is administered two months later. Each dose is three micrograms, one-tenth of the adult dose. An early analysis suggested the vaccine was 80 percent effective against symptomatic illness.
The pediatric trials for both vaccines were not primarily designed to measure whether the shots prevented symptomatic illness. Instead, following a regulatory path often used to expand vaccine eligibility into younger age groups, scientists measured the levels of virus-blocking antibodies in children’s blood and compared those measurements to the levels that were protective in young adults.
For all the pediatric age groups, the FDA said there was uncertainty surrounding the duration of vaccine effectiveness, which has waned over time in adults. In addition, the agency said based on experience with adults “it is likely that a booster dose will be needed to increase robustness, breadth, and duration of protection against currently circulating and emerging SARS-CoV-2 variants.”
Moderna had requested permission to use its vaccine in adolescents more than a year ago, but that authorization was held up by concerns about the risk of rare cardiac side effects — inflammation of the heart muscle and surrounding tissue — called myocarditis and pericarditis. Both Moderna and Pfizer-BioNTech vaccines have been linked to the heart problems in young adult males. Most cases are mild and inflammation caused by covid-19 tends to be more severe.
In the new briefing documents, the FDA said there were no confirmed cases of myocarditis or pericarditis in the Moderna trials for infants, children and adolescents.
In a submission to the FDA, Moderna said it has begun testing booster shots in all pediatric age groups. The ones for children under 6 will be the original vaccine or the company’s new bivalent version that also targets both the original strain and the omicron variant.
Once available, vaccines for the youngest children are unlikely to be immediately embraced by most parents. Fewer than 20 percent of parents say they plan to get their infants and young children immunized immediately, according to a Kaiser Family Foundation survey.
“There will be two types of parents: ones that will really embrace the vaccines and others who are going to wait and see” how other children do, said John P. Moore, a professor of microbiology and immunology at Weill Cornell Medicine.
Moore said that many parents of young children have been influenced by vaccine misinformation partly because the risks to children from the coronavirus are relatively slim.
“It can be serious for children, but that’s very rare,” Moore said. “It’s very different for Granny and Granddad, who are in a much higher risk group. For them, it is a no-brainer.”
Vaccines for young children have followed a twisting — and often confusing — path, marked by disappointing results, delays and changes in regulatory strategies.
Users browsing this forum: No registered users and 21 guests