Dismantling The Covid Pandemic & mRNA “Vaccine” NarrativesA podcast debut
JONATHAN ENGLER AND MARTIN NEIL
AUG 4, 2023
...
Dr Malik and I divided the podcast up into two distinct parts:
1. Did we actually have a lethal pandemic of a novel spreading virus?
2. How “safe and effective” are the mRNA “vaccines”?Part One: Did we actually have a lethal pandemic of a novel spreading virus?For part one, I should point out that I focused on the spring 2020 period only. This is not because what happened thereafter is not important, but because it is the period when the phase change from normal to abnormal occurred. As such it is the most instructive as regards the origin of the pandemic narrative. Later, the prolonged and hugely geographically variable effects of lockdowns, other interventions and the “vaccine” rollouts significantly complicate any analysis.
I started out by outlining one of my greatest current concerns, which is that many on “our side” of the debate are falling for a story which is, at best, a distraction, from the most important considerations.
“finally the truth about a lab-leak is coming out, and, finally, we know the true cause of the pandemic”.
I don’t agree with this sentiment.
In my view, the establishment is unlikely to have lost control over the mainstream media. It now appears to be allowing the lab-leak story to come out, and in fact even encouraging it. That is because it would much rather people pre-occupy themselves with the mystery of “where did it come from?” than they attempt to seriously address two questions:
“Is the SARS-CoV-2 virus actually relatively more lethal than the respiratory viruses that typically occur during winter?”, and
“If not then what caused all the deaths?”
The question as to whether the origin of SARS-Cov-2 was a lab or zoonotic is a classic “false dichotomy”, as I pointed out in this tweet. It’s a distraction, and one I explain in the podcast.
I then moved on to discuss why I considered that there had not actually been a lethal viral pandemic.
In doing so I revisit the early Spring 2020 period of the Covid era. At that time the pandemic narrative was driven by media reports of a huge number of all-cause excess deaths emerging from a small number of geographically separate places, most notably Northern Italy and New York City.
Furthermore, assumptions made about the lethality of “the virus” emerged in large part because of what happened in these places, and these then drove the global fear response.
But does this story actually stack up?
In the podcast, I delved into the constituent elements making up the establishment narrative, these being:
That the virus was novel (meaning we had no prior immunity and “everyone was susceptible”) - but if it was, how come so few people (eg on the Diamond Princess) became ill?
That it was particularly deadly - but how well do the steep rise in all-cause excess death reports in New York (a higher death rate in some weeks than in “Spanish Flu”) sit with the published work of John Ioannidis, who estimated the lethality to be in the ballpark of seasonal flu? (In the podcast I explain why even this figure is likely overestimated).1
That the steep rise in all-cause excess death reports were caused directly by a spreading virus - if so, why is there no real evidence of “spread” (E.g., in one of the “epicentres” - Lombardy, Italy) and how could whatever “it” was had been spreading for so many months in so many places without causing any observable all-cause excess deaths?
In terms of further reading in relation to the above, this article which I co-authored for PANDA lays out evidence relating to novelty and lethality, and this article discusses further whether there was evidence of “viral spread” linked to all-cause excess deaths in Northern Italy.
One important point I tried to make in the podcast which some people forget is that the establishment narrative relies on all parts of their story being true: that a novel and lethal virus to which we had no immunity spread from Wuhan directly causing waves of all-cause excess deaths, that propagated throughout the world.
If any part of this narrative is untrue, then what we are being told is a lie.
For instance, I sometimes hear people say: we had a pandemic, but it turned out to be little worse than flu. To that I say: we weren’t sold a wave of flu-like illness. No, the justification for a reordering of society and coerced or forced rollout of a novel gene therapy wasn’t a mild flu-like virus, it was a deadly novel one.
During the podcast, I am sorry that I failed to pay tribute to my PANDA colleague Jessica Hockett (who tweets as @EWoodhouse7 and has a substack here), who has done some amazing work drilling into the historical data for New York City.
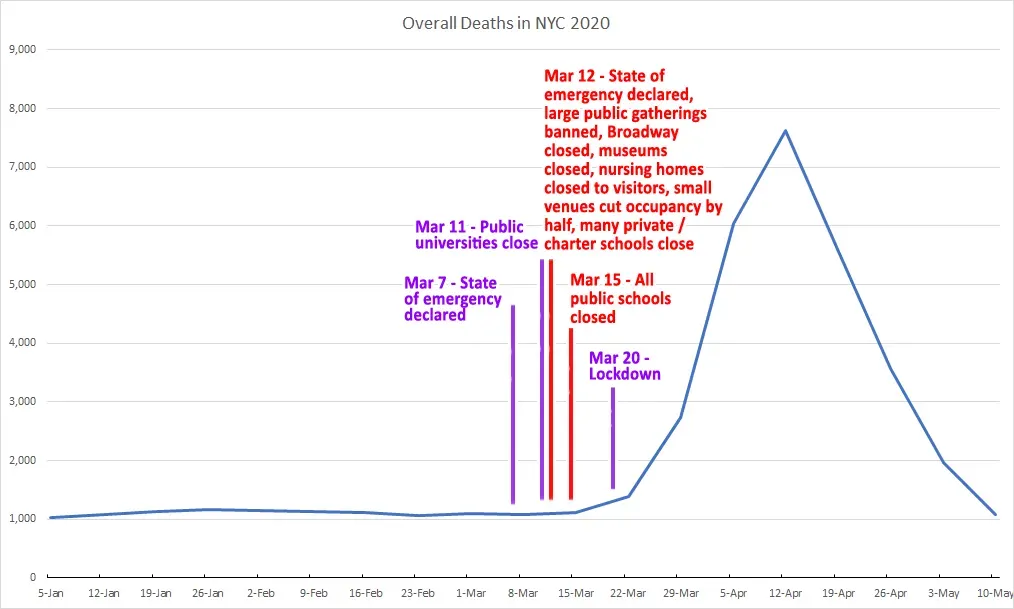
Whereas Ioannidis put the IFR of SARS-CoV-2 in the ballpark of seasonal flu, the crude mortality rate graph for New York City going back to 2015 looks like this:
That story is that:
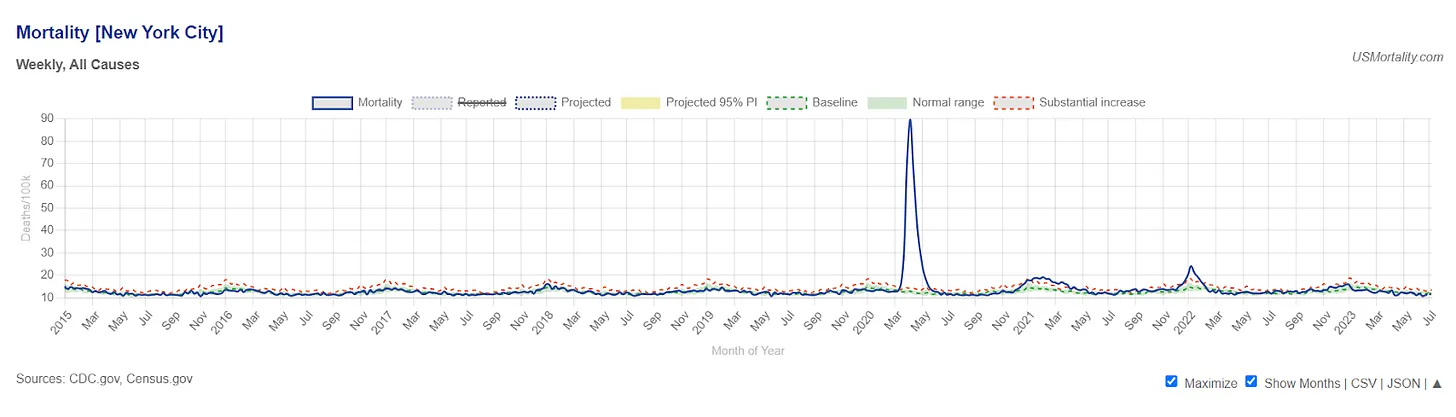
Whereas prior flu seasons register barely a ripple, for a few short weeks in 2020 the number of people dying is many multiples of the prior typical seasonal peaks, with a zenith during week 15 at around a huge 600% increase. Moreover, and unlike that seen in other places, this increase is seen in the young and middle aged as well as the elderly.
As Jessica has described (E.g., in this highly recommended conversation with JJ Couey), this bears no relation to what would be expected by the spread of any virus, let alone one which we now know was essentially flu-like in its lethality.
Instead, this sharp peak looks like the sort of mortality increase from a “mass casualty event” such as a terrorist attack. I have little doubt that - whilst the details are yet to be elucidated - there are huge untruths in what we are being told about what happened in New York City, yet what we have been told happened there, as well as in Lombardy and in Madrid, Spain, was used to convince the rest of the world that the SARS-CoV-2 virus was lethal.
I recommend you keep a look-out for Jessica’s additions to her series on New York City at her substack here.
In the next part of the podcast I went on to discuss the range of catastrophic measures implemented, and how these could themselves have resulted in the deaths observed. I cover some of the same ground as covered in the Northern Italy article mentioned above, from which this is an extract:

Of course, since writing the above, evidence of a number of other harmful interventions has emerged which were mentioned during the podcast, including:
Overuse of midazolam and opiates as encouraged by the now infamous NICE document NG163 (deleted but accessible here), which essentially copied treatment guidelines which may be appropriate for terminally ill cancer patients into those for patients with respiratory infections. Martin Neil and Norman Fenton expand on this (and some other matters) here.
Large falls in the use of antibiotics (E.g., in the USA, and also recorded in the UK and Australia) as a standard therapy for those with a “chest infection”, especially the elderly. This may have been particularly harmful given the fact that when people die following respiratory viral infection it is invariably from secondary bacterial infection, not the direct effects of whatever virus initiated the episode of illness. This is something that even the US Covid response guru Dr Anthony Fauci has previously stressed. In his 2008 article in the Journal of Infectious Diseases (which reported on autopsies of well-preserved victims of the Spanish Flu pandemic) he concluded that:
“Prevention, diagnosis, prophylaxis, and treatment of secondary bacterial pneumonia, as well as stockpiling of antibiotics and bacterial vaccines, should also be high priorities for pandemic planning.”Face-coverings can be hazardous given that potentially pathogenic bacterial colonies can easily contaminate them (as were found on nearly every face covering used by a series of volunteers when examined in a study in Japan, as reported in Nature). The severity of the bacterial hazard naturally increases when masks are used by the immuno-compromised (such as the elderly), who might then develop a bacterial infection, which itself could be left untreated since antibiotics might have been denied in the presence of a positive covid test.
In relation to the last two points above, it has been suggested that secondary bacterial pneumonia was only present in a small proportion of those classed as “covid deaths”. Though, it is unclear why Fauci’s conclusions about the Spanish flu:
“….the majority of deaths in the 1918–1919 influenza pandemic likely resulted directly from secondary bacterial pneumonia caused by common upper respiratory-tract bacteria”.
would not be substantially the same for another virus causing flu-like illness.
One important part of the official narrative which I did not have time to cover was that of the magical disappearance of flu. Martin Neil covered this in his podcast with Ahmad, and this is well worth a listen. (Spoiler alert: changes in human behaviour, especially related to testing, were probably the main cause of the illusion of the vanishing flu.) I actually contributed to several of the articles which Martin has written on this topic, which can be found here.
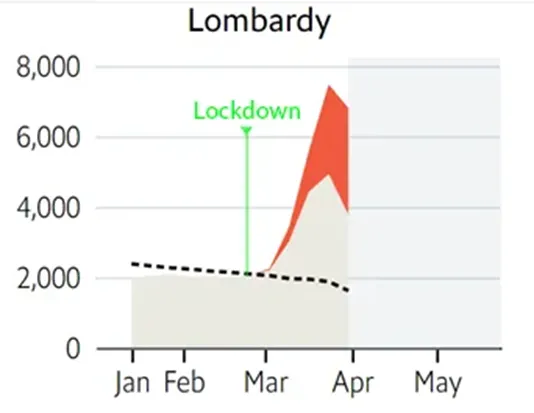
Before moving onto the second part of the podcast, it is worth pointing out that a number of people previously elucidated that the harms must have been response-driven rather than caused by a deadly virus, and it is to my chagrin that I (and other colleagues) did not take these theories seriously enough at an early enough stage in the ‘pandemic’.
For example, someone writing by the name of John Pospichal posited in May 2020 that the all-cause excess death curves invariably followed - rather than preceded - the imposition of lockdowns, generating the default hypothesis that the measures caused the deaths, yet nobody seems to have picked up on this at the time. For example, here is Pospichal’s chart for Lombardy:
Furthermore, the Canadian scientist Denis Rancourt has written extensively on this theme, publishing his first article, titled “All-cause mortality during COVID-19 - No plague and a likely signature of mass homicide by government response”, and did so as early as June 2020.
More “respectable” scientists (and I use that term ironically) also seem to have uncovered clues throughout the past few years. For example, in this paper out of New York published in December 2020, the authors conclude - apparently without appreciating that it essentially obliterates the “sudden spreading virus” story - that:
“Our data reveal that SARS-CoV-2 incidence emerged rapidly and almost simultaneously across a broad demographic population in the region. These findings support the premise that SARS-CoV-2 infection was widely distributed prior to virus testing availability.”
The fact that it appeared to emerge simultaneously across multiple locations, rather than spread from a small number of points of origin, is starkly illustrated by this video posted by the authors:
[video clip at source]
Finally, if it’s not obvious, it’s worth reiterating why I am so fixated on the question as to whether we actually had a pandemic, and what dangers attach to the (false) notion that we had a dangerous lab-leak.
The answer to this is two-fold:
Firstly, huge harms have been wrought on the world’s population based on the assumption that we had a global problem requiring a top-down centralized global solution. In my view that’s a dangerous notion in itself, easily twisted and usable by bad actors with control over the media for a variety of purposes which may not be totally benign.
Secondly, and more specifically related to “viruses”, whereas the likely proposed solution (centralized, top-down of course) to the “lab-leak” will be some sort of ban / treaty on “gain of function”, this always leaves open the possibility that in future someone will claim (truthfully or not) that a leak has occurred, perhaps by a rogue nation or by a rogue scientist, and the same fear-porn driven nightmare could play out once again.
Of course, the truth is that leaks at biolabs happen rather frequently (and those are only the ones we know about), and whilst they may be capable of causing some local illness, the idea they could cause a global lethal pandemic owes more to the over-inflated views of a small number of scientists as to their state of knowledge and capabilities than to that which reality actually suggests.
Part 2: How “safe and effective” are the mRNA “vaccines”?As it turned out, we didn’t have time to drill into the question of efficacy, and only managed a discussion touching on safety.
However, in relation to efficacy, had I had time I would have referred to the main statistical illusion (of several) employed in the clinical trials and post-marketing “real-world studies” which create the illusion of efficacy: classification of individuals as unvaccinated for some period of time (usually 7, 14 or 28 days) after injection.
The many studies which have employed this trick are listed in this article by Martin Neil and Norman Fenton.
I would also have made a few additional points:
1. In a study of infection rates, the effect above is magnified (one could even say “boosted”!) by an active censoring process. By suppressing immunity, the injections might have made the recipient more vulnerable to infection shortly after vaccination. This would effectively pull-backwards infections that might have occurred naturally, but at some later point in time. Thus, infections in injection recipients would tend to be concentrated within this short period of time, rather than subject to the natural infection process. By censoring any reports of infections that occurred in this short period the reported infection rate in the injected would then be significantly smaller than the reported infection rate in those not injected.
2. In a study of deaths or hospitalizations, the capacity for such a policy to mislead - if vaccine-related events occurring soon after injection are simply ignored - is obvious.
3. Most analyses only examine “covid” related events (infections, hospitalisations and deaths). However, given (1) the inconsistencies and uncertainties around categorisation into “covid” and “non-covid” buckets, and (2) the significant and varied “off-target” effects of these products, the only reliable and meaningful analyses must surely utilise all-cause mortality data.
4. “Real-world” studies can be subject to selection biases such as unhealthy or healthy vaccinee bias (where the health of the vaccinated is worse/better than the unvaccinated) which is difficult to adequately correct for statistically. (This is one of the reasons we do randomised trials!)
In relation to the Clalit Health Services booster study from Israel published in the NEJM in Dec 2021 (which was highly influential worldwide),
a recent letter to the journal has pointed out that unreported healthy vaccinee bias actually accounts for all the claimed benefit of the injections. This is all the more shocking when it is appreciated that the original authors had access to data allowing them to make that conclusion yet failed to mention it at all.It should, of course, come as no surprise at all that a product which generates a fixed and specific blood-borne antibody to one discrete part of a highly mutable virus provides little clinically relevant protection, especially to “variants”. The heavy lifting in terms of defence against respiratory viruses takes place in the respiratory mucosa, as I described in this thread, and the body’s natural immune system is able to provide durable immunity which is, moreover, flexible enough to protect against variants of viruses it has encountered before.
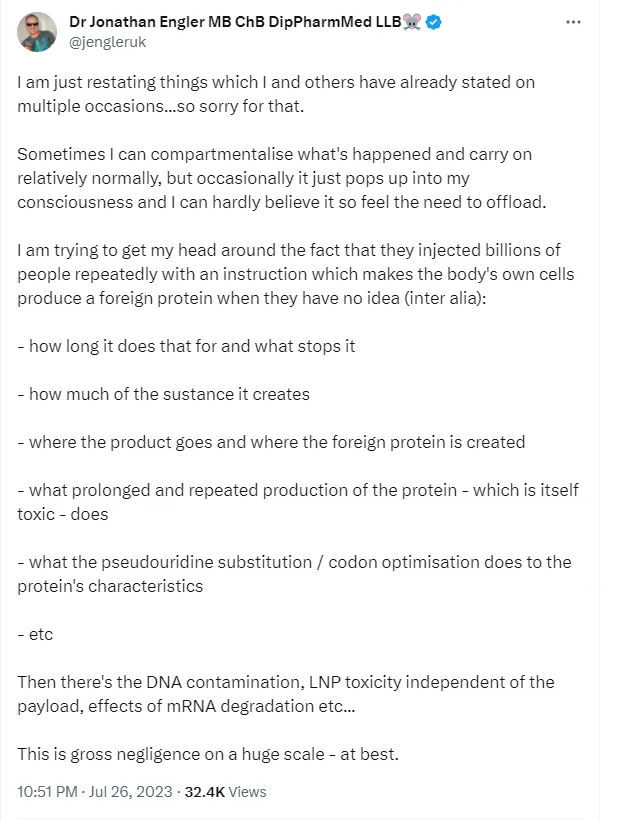
As regards safety, much of the material we covered is basically summarised by this tweet, and there’s little need to expand on it in this article:
In addition to the above, we also discussed the huge miss-step taken by regulators in allowing the mRNA products to proceed through an approval pathway usually applied to vaccines, on the (faulty) basis that the injected product was broken down entirely in the arm. This meant that certain studies required for “regular” drugs (e.g., pharmacokinetics, biodistribution, carcinogenicity, and fertility) were not required or provided.
I pointed out that:
1. In SEC filings required for financial regulatory purposes,
both Pfizer and Moderna considered their products to be gene therapies and identified this as a potential risk for investors as “the regulatory pathway for approval is uncertain”.2. A biodistribution study in rats, a report of which was prised out of the FDA as part of the litigation spear-headed by Aaron Siri (FDA / Pfizer had wanted the data hidden for 75 years)
showed that the product was widely distributed throughout the body after injection, and the regulators must have known this while they were insisting to the public that this was not the case. (See thread here.)
3. The
LNPs were originally designed with the function of carrying cancer drugs to their target, and as such were designed to cross membranes and become widely distributed.4. The wide range of adverse events received by Pfizer up to end-Feb 2021 (only a few months after rollout) suggested wide distribution. Of particular concern was the
1441 reports of a serious adverse event of special interest affecting the cardiovascular system, 946 of which were serious; these had a median onset of action of less than 24 hours after injection.(During the podcast I actually mistakenly referred to a figure of 1223 such events, which is actually - and no less disturbingly - the total number of fatal adverse events reported to Pfizer in that same cumulative safety report.)
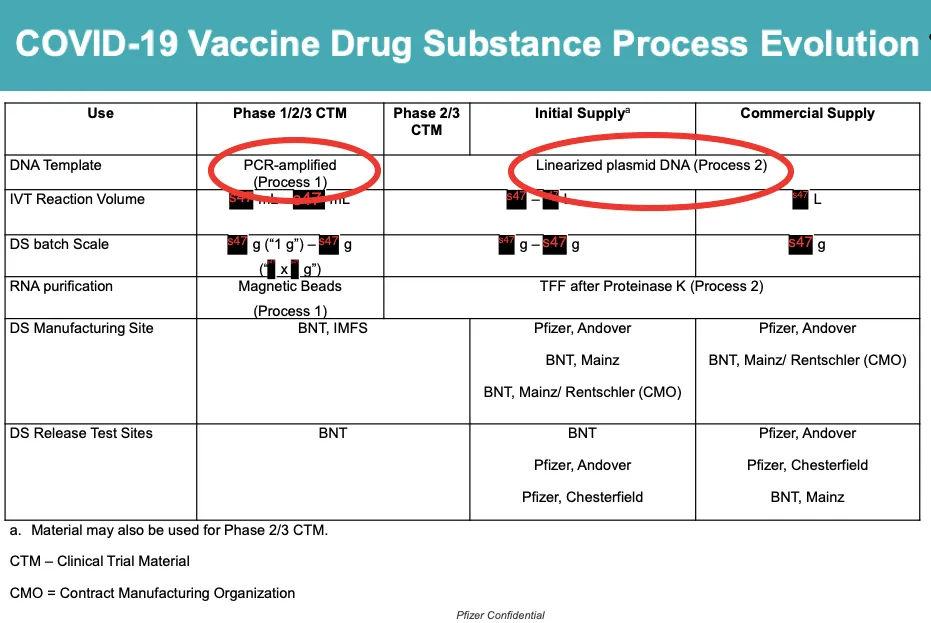
I did not get to discuss the DNA contamination or batch issues recently widely reported (mentioned in my tweet above), but to be honest there are others who know far more about that aspect of matters than I do.
Of course, the astonishment I express is all the more brought into focus by the points covered in the first part, in that not only are these injections unlikely to be safe by design, but if there was no real pandemic, they weren’t even needed,
which makes the coercive rollout all the more egregious.ConclusionBy way of conclusion,
I should reiterate that the evidence suggests that there was no pandemic in 2020, by any reasonable definition of that word. All the harm observed since spring 2020 was caused by the dystopian response to the perceived threat, including the rollout of a number of “vaccines” which were neither safe nor effective.I hope this article has given you a sufficient taster of the material covered to make you want to listen to the podcast. Any feedback is most welcome.