What is the evidence for these assertions?
This is a statement often made in response to concerns raised about the incidence of myocarditis after the mRNA injections. The source of this has been a number of deeply flawed papers, the most recent of which was a “systematic review and meta-analysis” published in Frontiers. This claimed a 7-fold difference between myocarditis risk after infection vs mRNA vaccine.
The claim – which contradicts several other studies, including this massive Nordic study covering 23m subjects published in JAMA– has been expertly analysed in [this Twitter thread by @sborg40](https://threadreaderapp.com/thread/1582 ... 81377.html), an account with a profile of “Retired Infectious Disease Physician”.) – has been expertly analysed in this Twitter thread by @sborg40, an account with a profile of “Retired Infectious Disease Physician”.
A meta-analysis is a method whereby the data from many different studies are combined into one analysis. The idea is that by increasing the number of subjects covered, the results are more reliable and representative and hence statistically more powerful. However, the outcome of such an analysis is entirely dependent on (amongst other things) the studies which are used, and in fact the main criticisms of the Frontiers paper relate to the specific studies selected.
For the paper, the authors found 763 potentially relevant studies but whittled these down to only 22 (3%) for inclusion in the analysis. The Twitter thread lists the shortcomings identified which we do not intend repeating here, but in brief some of the issues @sboprg40 found with the studies which were considered for the analysis were:
* 3 of the 10 studies of myocarditis after covid had evidence of bias compared to none of the 12 studies after vaccination
* One study was conducted by the CDC without peer review, this study looking only at the hospitalised and failing to examine all those infected
* Some studies were conducted in the elderly, in ITU patients and severe covid with accompanying non-specific cardiac damage
* Myocarditis diagnoses were accepted by authors without specific diagnostic criteria, in one study diagnoses were merely “probable”
* Covid diagnoses were not consistent and reliable
Overall therefore, this meta-analysis contributes little to answering the core question of interest: does mRNA vaccination in the healthy young population increase the risk of myocarditis at all, and if it does how does it compare to the risk from a covid infection?
One of the most comprehensive studies looking at the risk of myocarditis after covid infection was this study out of Israel (which has an advanced and comprehensive electronic medical records system), covering a large population of nearly 200k subjects.
The authors “did not observe an increased incidence of either pericarditis or myocarditis in adult patients recovering from COVID-19 infection”. Heath Advisory and Recovery Team: Myocarditis began with vaccine rollout
This is, of course, entirely consistent with what is the strongest (and also simplest) evidence against the core claim, which is that numerically an increase in myocarditis cases simply wasn’t a feature of 2020, but rather this started in 2021.
Figure 1: Incidence of myocarditis across 40 hospitals in USA

https://jamanetwork.com/journals/jama/f ... le/2782900
...
Heath Advisory and Recovery Team: Myocarditis began with vaccine rollout
More data to back up myocarditis concerns
There are two key points regarding post vaccination heart issues that HART have been raising concerns about since early 2021.
* Myocarditis is attributable to injection not infection
* What has been diagnosed may represent wider harm that is yet to be properly measured
...
Many people have claimed that it is the virus that is the underlying cause for myocarditis rather than the vaccinations. There are several ways to check this hypothesis. The obvious one is to compare the rate of myocarditis after infection in:
a) uninjected uninfected
b) uninjected infected
c) injected uninfected
d) injected infected
Although there have been several epidemiological analyses of myocarditis, that simple comparison is never made. Where uninjected people are looked at specifically, there is no evidence of an increase in incidence. HART has previously summarised the data after infection in the injected compared to the uninjected.
An alternative approach is to look at how common myocarditis is over time. Did the incidence increase with the arrival of covid in 2020 or the arrival of injections in 2021?
There are now several sources of data to answer that question and they all concur.
...
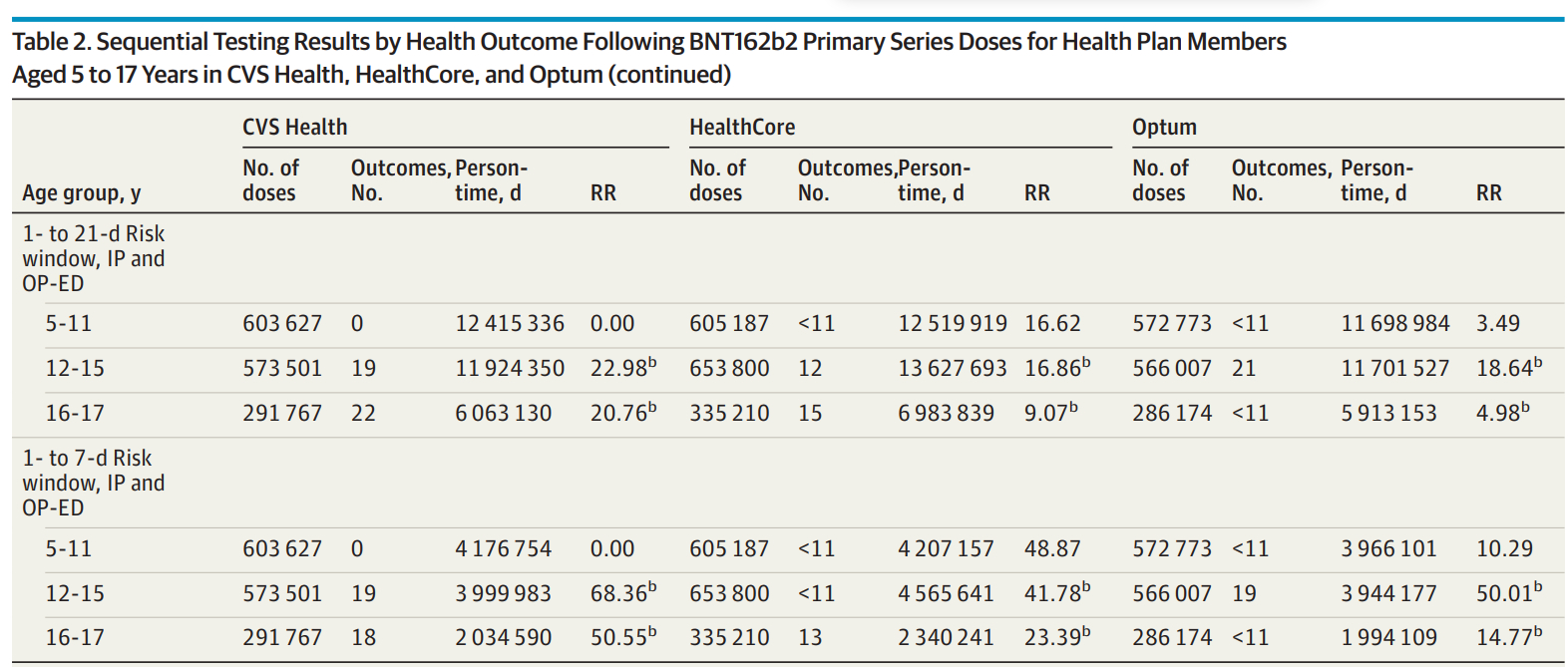
All three studies demonstrate a far higher rate of subclinical harm from injection than the rate measured when only looking at hospitalisations that result in a myocarditis or pericarditis diagnosis.
...
Heath Advisory and Recovery Team: Myocarditis concerns grow
HART has been trying to raise awareness for over two years.
A new study performed on adolescents in Hong Kong who suffered myocarditis after mRNA injection in Circulation appears to be generating quite a lot of discussion over how common it is, and what the long-term outcomes are for those unfortunate enough to suffer from this side effect.
Broadly speaking, the more we learn, the worse it looks.
...
Since then, we have also written about further worrying data emerging, especially regarding subclinical cases which are only found by measuring troponin levels systematically. This is logistically simple to perform, so it is criminal that it wasn’t done as soon as the signal of potential harm emerged.
...