Joe Hillshoist » Sat May 22, 2021 8:20 pm wrote:Belligerent Savant » 21 May 2021 05:12 wrote:stickdog99 » Thu May 20, 2021 12:59 pm wrote:Joe Hillshoist » 20 May 2021 00:08 wrote:Belligerent Savant » 20 May 2021 03:52 wrote:.
Sliding this in here in the interim:@ianmSC
·
Back on 1/27, scientist Eric Topol said the UK variant “beast” was going to create a 4th surge & that we should enforce wearing N95 masks to stop it
After he was proven completely wrong, he tweeted yesterday: “who thinks scientists are always getting it wrong?”
https://twitter.com/ianmSC/status/13950 ... 08512?s=20
This is worthy of a read as well, for those inclined:
https://ianmsc.substack.com/p/follow-th ... ce=twitter
Does that graph just show the vaccine essentially works to curb the spread of COVID?
Basically the sharp peak and drop, which is the most defined sharp peak in the whole image, starts two to three weeks after the vaccine rollout began and has continued as a trend since, for the first time since early 2020.
OK, that's an interesting theory. Now where are the hard data to back this theory up?
I already replied to this earlier, but the drops also strongly coincide with the seasonal nature of flu variants. We saw the same/similar drops last year around the same time, as flu season ends.
There's also been increases in cases after vaccination in certain regions, and many instances of those vaccinated testing positive again.
These shots do NOT "immunize". All they claim to do -- once again -- is minimize symptoms.
I don't think you know what you are talking about when you say "These shots do not immunise all they claim to do is minimise symptoms."
However why don't you show the data in graph form of previous flu seasons including the similar almost cliff like drop in death rates from early/mid winter that the graph above shows. Because there aren't any that I can find and again this leads me to think you are wrong about this.
The closest is the 2015/16 season. But at no time in the last 5 years has the flu season death rate dropped so significantly during the first weeks of the year. The earliest decline so far with the flu death rate is mid February but its usually late March. Ie into Spring, not early winter.
Therefore there is no relationship between that graph and flu deaths.

Are you putting forth the claim that the vaccines are the cause for the drop? Because there are many charts that infer the opposite. Herd immunity is a real thing, and if there's any prominent reason for the likely drop, it's the combination of herd immunity/percentage of the population that have already been infected, and also the potential benefit of lessened symptoms from a number of those vaccinated (those that didn't test positive or die after vaccination, that is), along with seasonal drops, though it's difficult to say with certainty right now as the data has largely been misleading from the start (the manner in which a "case" has been defined since the onset of covid; the manner in which "deaths" have been defined since the onset of covid, etc. -- the criteria for tallying both of these figures, and others, are unprecedented when compared to methods employed PRIOR TO 2020).
It may well be this virus has been essentially a non-factor -- i.e., countries have already largely reached herd immunity -- in most countries, for months (especially when considering the percentage of false-positive results for PCR tests with high cycle thresholds), and that any recent increases in cases and related deaths are materially due to these experimental shots.* A speculative take at this time, to be sure.
Side-bar:
*noteworthy development:
https://off-guardian.org/2021/05/18/how ... ctiveness/
How the CDC is manipulating data to prop-up “vaccine effectiveness”
New policies will artificially deflate “breakthrough infections” in the vaccinated, while the old rules continue to inflate case numbers in the unvaccinated.
It'll be months, or years, before there's clarity on this.
As far as what these shots actually claim to do, here's an excerpt direct from the FDA specific to the Pfizer shots:
https://www.fda.gov/media/144414/download
EMERGENCY USE AUTHORIZATION (EUA) OF THE PFIZER-BIONTECHCOVID-19 VACCINE TO PREVENT CORONAVIRUS DISEASE 2019(COVID-19)IN INDIVIDUALS 12YEARS OF AGE AND OLDER
You are being offered the Pfizer-BioNTech COVID-19 Vaccine to prevent Coronavirus Disease 2019 (COVID-19)caused by SARS-CoV-2. This Fact Sheet contains information to help you understand the risks and benefits of the Pfizer-BioNTech COVID-19 Vaccine, which you may receive because there is currently a pandemic of COVID-19. The Pfizer-BioNTech COVID-19 Vaccine is a vaccine and may prevent you from getting COVID-19. There is no U.S. Food and Drug Administration (FDA) approved vaccine to prevent COVID-19.
Read this Fact Sheet for information about the Pfizer-BioNTech COVID-19 Vaccine. Talk to the vaccination provider if you have questions. It is your choice to receive the Pfizer-BioNTech COVID-19 Vaccine.The Pfizer-BioNTech COVID-19 Vaccine is administered as a 2-dose series, 3 weeks apart, into the muscle. The Pfizer-BioNTech COVID-19 Vaccine may not protect everyone. This Fact Sheet may have been updated. For the most recent Fact Sheet, please see http://www.cvdvaccine.com.
WHAT IS THE PFIZER-BIONTECHCOVID-19 VACCINE?
The Pfizer-BioNTech COVID-19 Vaccine is an unapproved vaccine that may prevent COVID-19.There is no FDA-approved vaccine to prevent COVID-19.
...
WHAT SHOULD YOU MENTION TO YOUR VACCINATION PROVIDER BEFORE YOU GET THE PFIZER-BIONTECHCOVID-19VACCINE?
Tell the vaccination provider about all of your medical conditions, including if you:
•have any allergies
•have a fever
•have a bleeding disorder or are on a blood thinner
•are immunocompromised or are on a medicine that affects your immune system
•are pregnant or plan to become pregnant
•are breastfeeding
•have received another COVID-19 vaccine
•have ever fainted in association with an injection
...
WHAT ARE THE INGREDIENTS IN THE PFIZER-BIONTECH COVID-19 VACCINE?
The Pfizer-BioNTech COVID-19 Vaccine includes the following ingredients: mRNA, lipids ((4-hydroxybutyl)azanediyl)bis(hexane-6,1-diyl)bis(2-hexyldecanoate), 2 [(polyethylene glycol)-2000]-N,N-ditetradecylacetamide, 1,2-Distearoyl-sn-glycero-3-phosphocholine, and cholesterol), potassium chloride, monobasic potassium phosphate, sodium chloride, dibasic sodium phosphate dihydrate, and sucrose.
...
More at link. By the way, for those that received the Pfizer shots, were you provided the above info in advance?
There is no mention of 'immunization'. No details on what the shot may actually do other than indicating it "may" prevent one from getting COVID-19.
I also recommend reading through the following piece, titled: Synthetic mRNA Covid vaccines: A Risk-Benefit Analysis:
https://off-guardian.org/2021/02/22/syn ... -analysis/
An excerpt:
The Covid synthetic gene therapy injections employ synthetic, thermostable nucleotide sequences which are wrapped in a PEG (polyethylene glycol)-lipid nanoparticles to protect from destruction in the bloodstream and facilitate entry into the cells. The claim is that the cellular machinery will engage with these synthetic sequences and produce segments which code for the SarsCov2 S1 spike protein. It is believed that the immune system will mount a sufficient antibody response.
Dr David Martin, emphasized that this technology does not meet the definition of a traditional vaccine as per the manufacturers’ claims. The trials do not test for reduction in transmission. These therapies do not prevent infection, merely reduction in one or more symptoms.
Interestingly, Moderna describes its technology as the “software of life,” not a vaccine.
Also: the following link, shared by Stickdog in the mRNA thread, is worth reviewing as well, as it displays a number of charts across regions that suggest increases in deaths/cases in parallel with increase in vaccination:
https://threadreaderapp.com/thread/1387 ... 12324.html
Important #COVID19 vaxxine data thread. I have avoided tweeting about the vax issue as it’s become an immensely toxic topic. But there are some extremely worrying trends emerging between CV19 cases, deaths, & vaxxine administration.
Here, I will share publicly available data for #COVID19 vaxxinations, cases, & deaths in 17 countries + #Ontario & ask questions, as per the scientific method. You are free to make up your own mind regarding the trends shown.
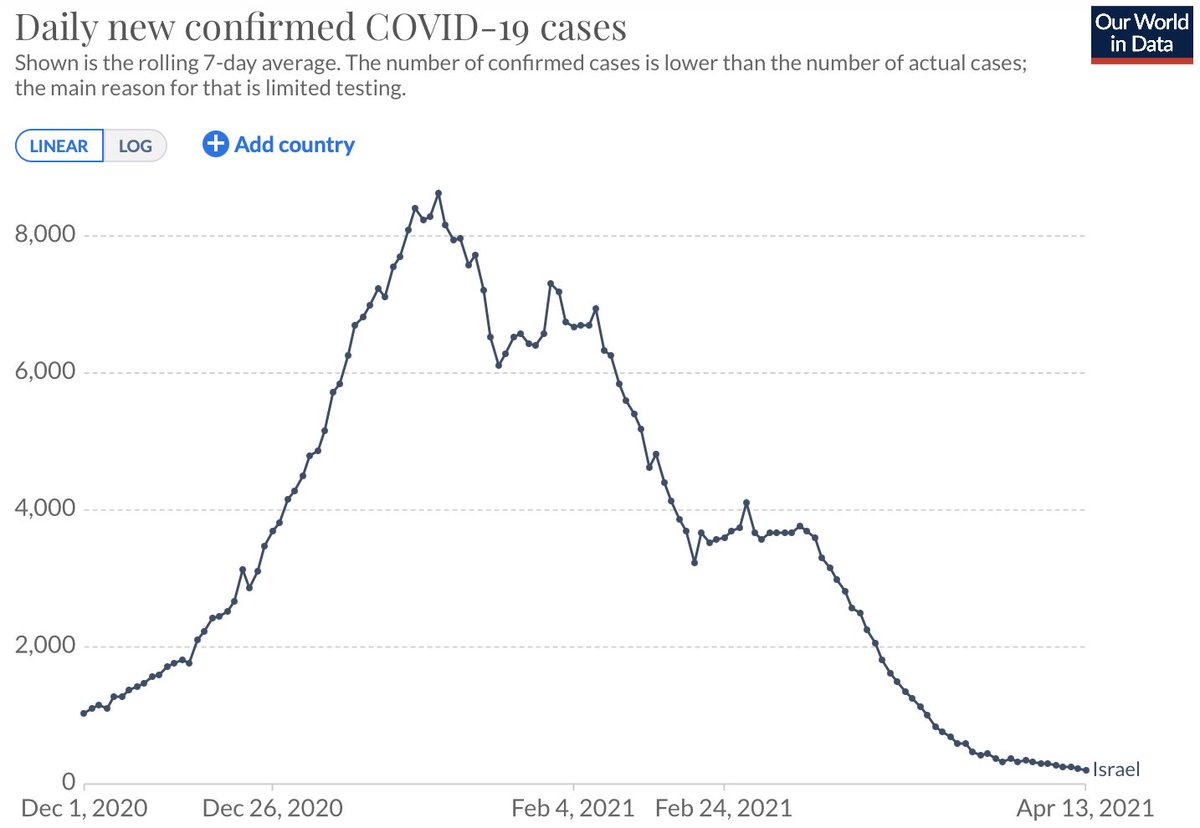
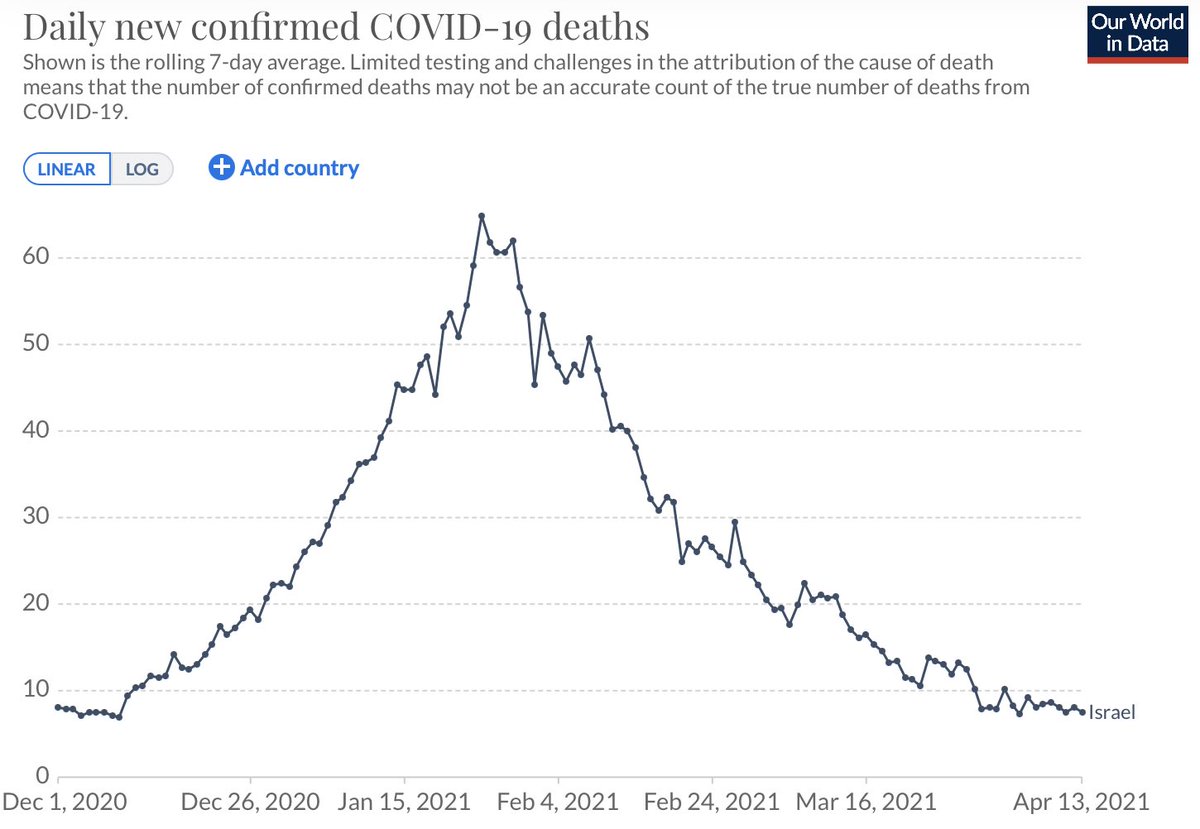
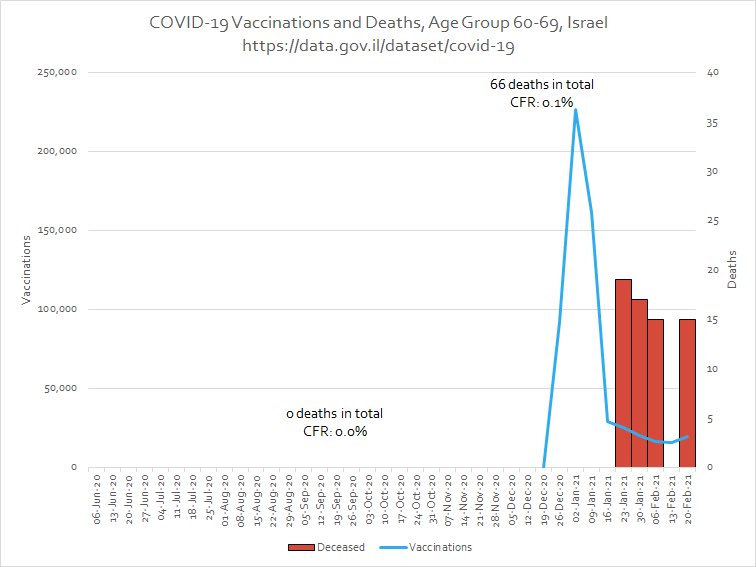
#Israel was the one of the first countries to start CV19 vaxxinations (19-Dec-2020). Since vaxxinations began, both CV19 cases & deaths continued to increase for ~5 weeks. It took 3 months for cases+deaths return to pre-vax levels.
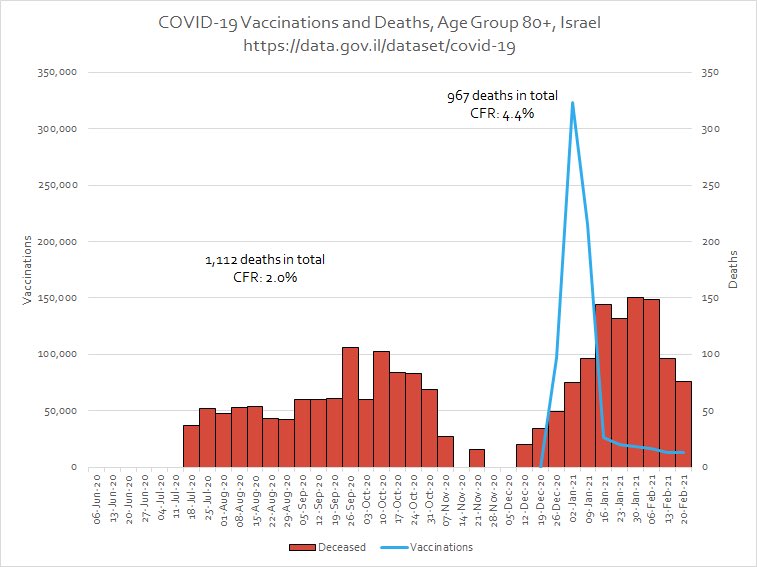
CV19 vaxxinations in #Israel are also associated w/ staggering increases in death for a month, as shown via CFR:
Age specific CFR changes post-vax (1 month):
80+: 220%
70-79: 600%
60-69: 0 deaths pre-vax, 66 deaths post-vax
...
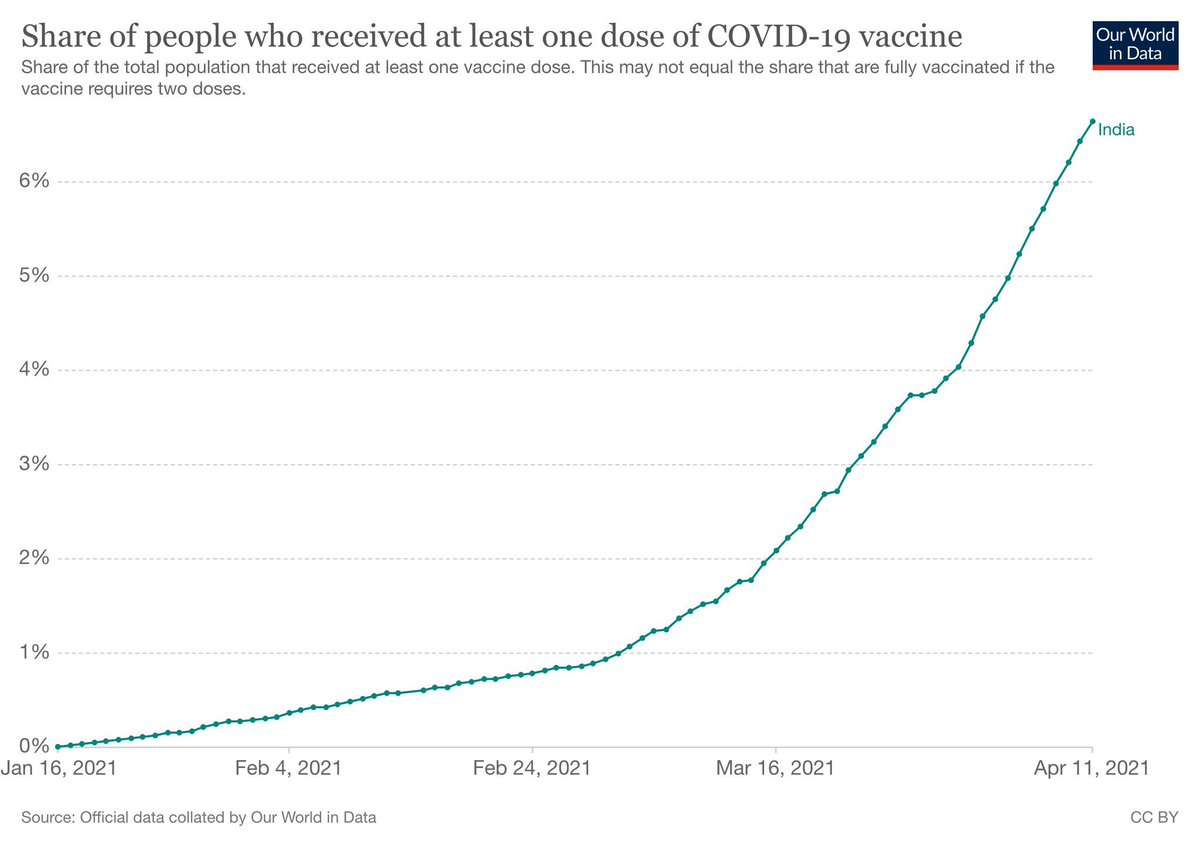
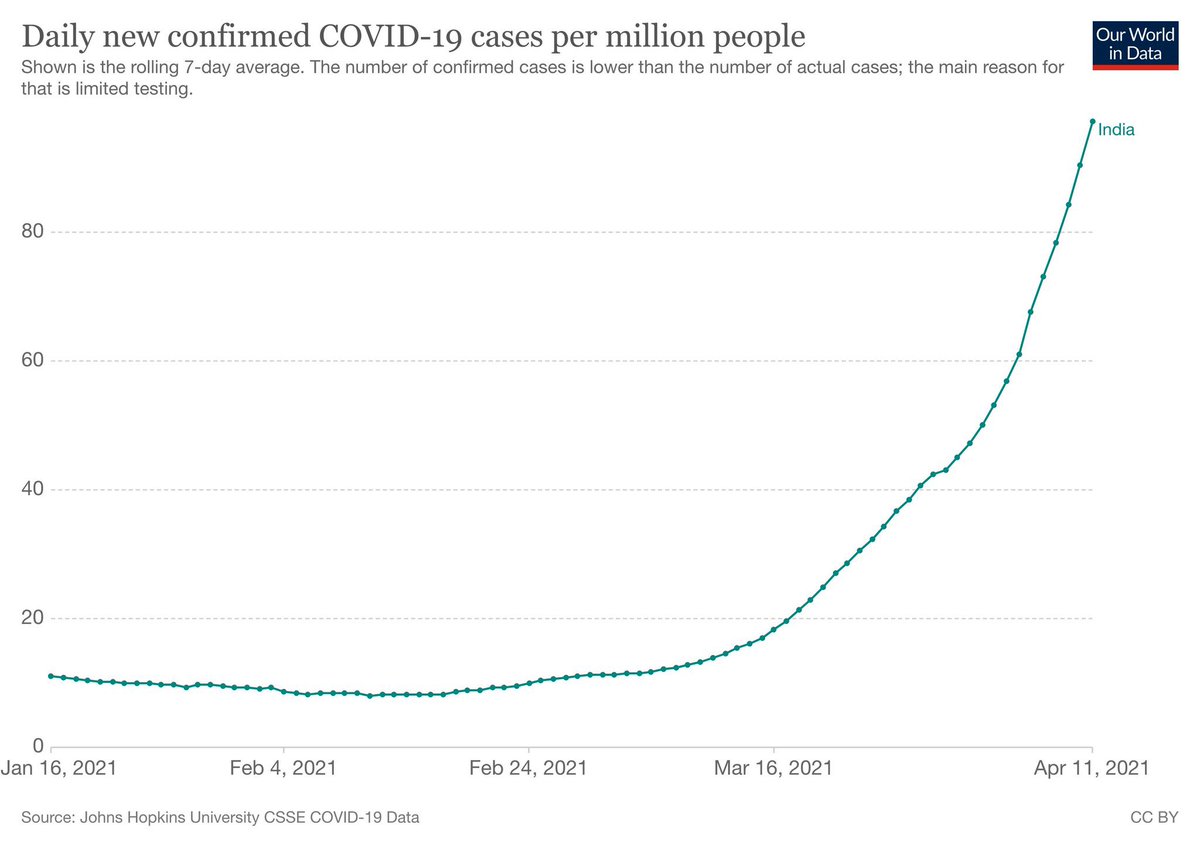
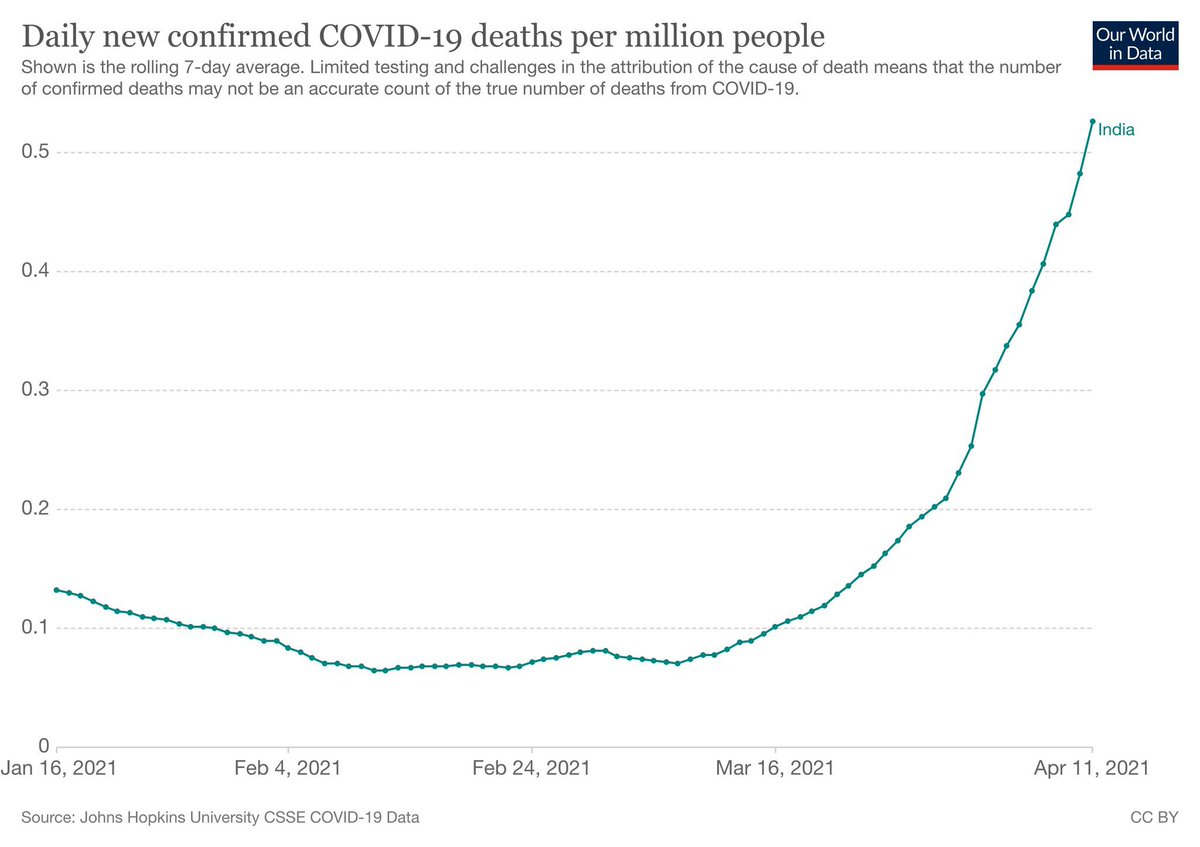
India is experiencing a significant increase in both CV19 cases & deaths these days. The graphs of CV19 cases, deaths, & share of people receiving their first vaxxine dose are virtually indistinguishable
...
If seasonality was causing an increase in the rising of CV19 cases & deaths, then these neighbouring countries would also be affected. The data so far shows that CV19 cases + deaths rise as a result of increasing vaxxinations.
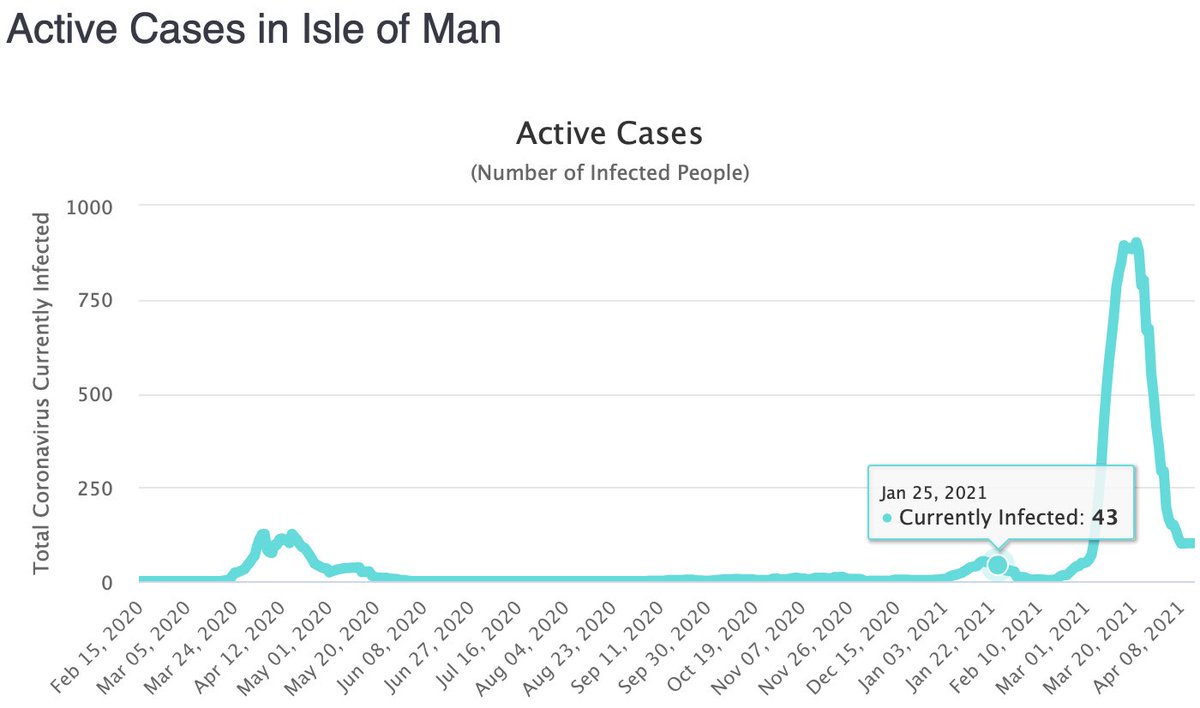
But the perfect case study would be if a nation, preferably an island (isolated/no land borders), that had very little to no CV19 cases prior to vaxxinations, experienced a big jump in infections#s post-vax. Luckily, there are 3 we know of:
The Isle of Man started administering vaxxinations on 25-Jan-2021. Prior to this, there were little to no CV19 infections, but a sharp increase in cases is seen as vaxxinations began
The island of Bonaire started it’s vaxxinations on 22-Feb-2021. It too, saw a significant increase in both CV19 cases & deaths after vaxxinations began. CV19 cases & deaths were low before vaxxinations began:
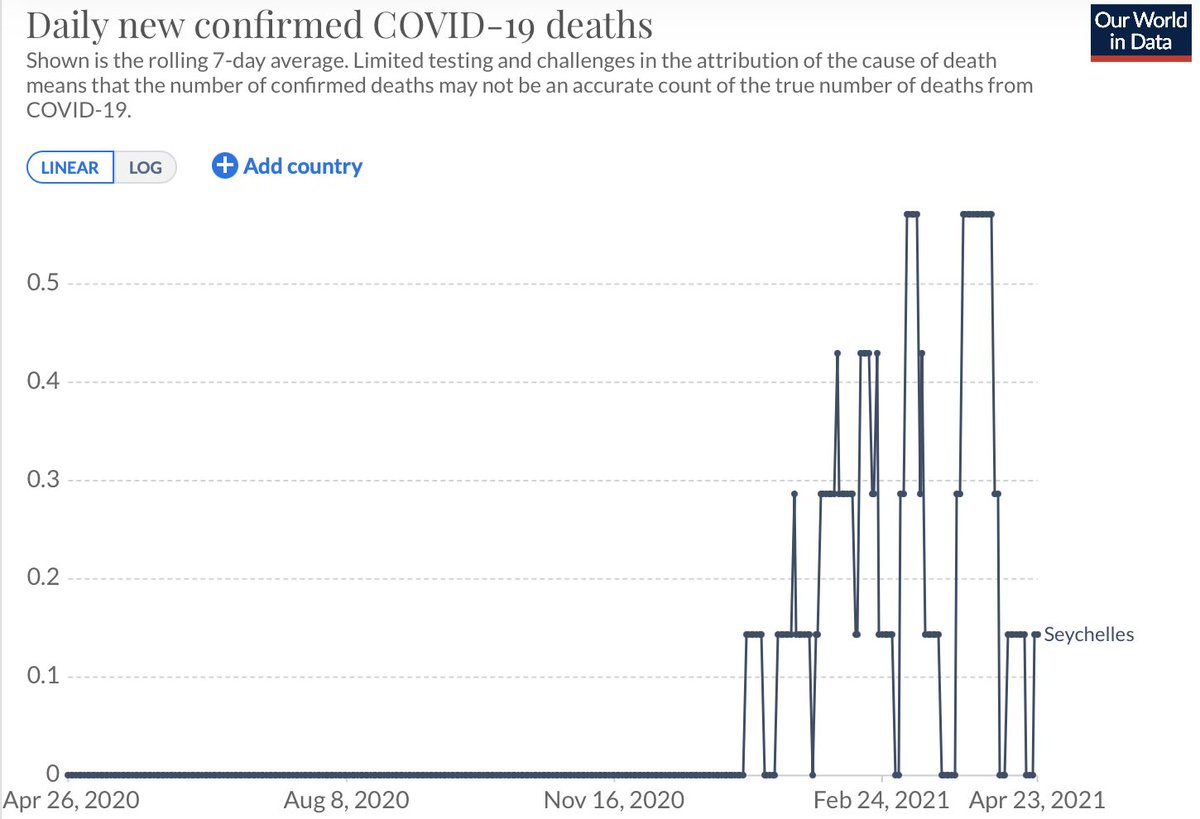
Finally, the island of Seychelles, also saw a steep rise in both CV19 cases & deaths after vaxxinations started, & numbers of cases & deaths haven’t returned to pre-vax levels even after 3 months of vaxxinations:
But these trends are not only seen on island nations, which are arguably the best case studies to show effects of vaxxinations on CV19 cases & deaths. This exact same trend is also seen in Cambodia, Thailand, & Laos. So how do we explain these data if it’s not seasonality?
So a question that must be asked is:
Are vaxxines responsible for these rises in CV19 cases & deaths (3rd wave)? If they are, is there any evidence that vaxxinated people are:
a) getting CV19, and
b) being hospitalized/in ICUs?
There is actually a great deal of evidence, both anecdotal as well as in the published scientific literature, to show that vaxxinated people can get CV19. Even the #CDC has openly admitted this as well
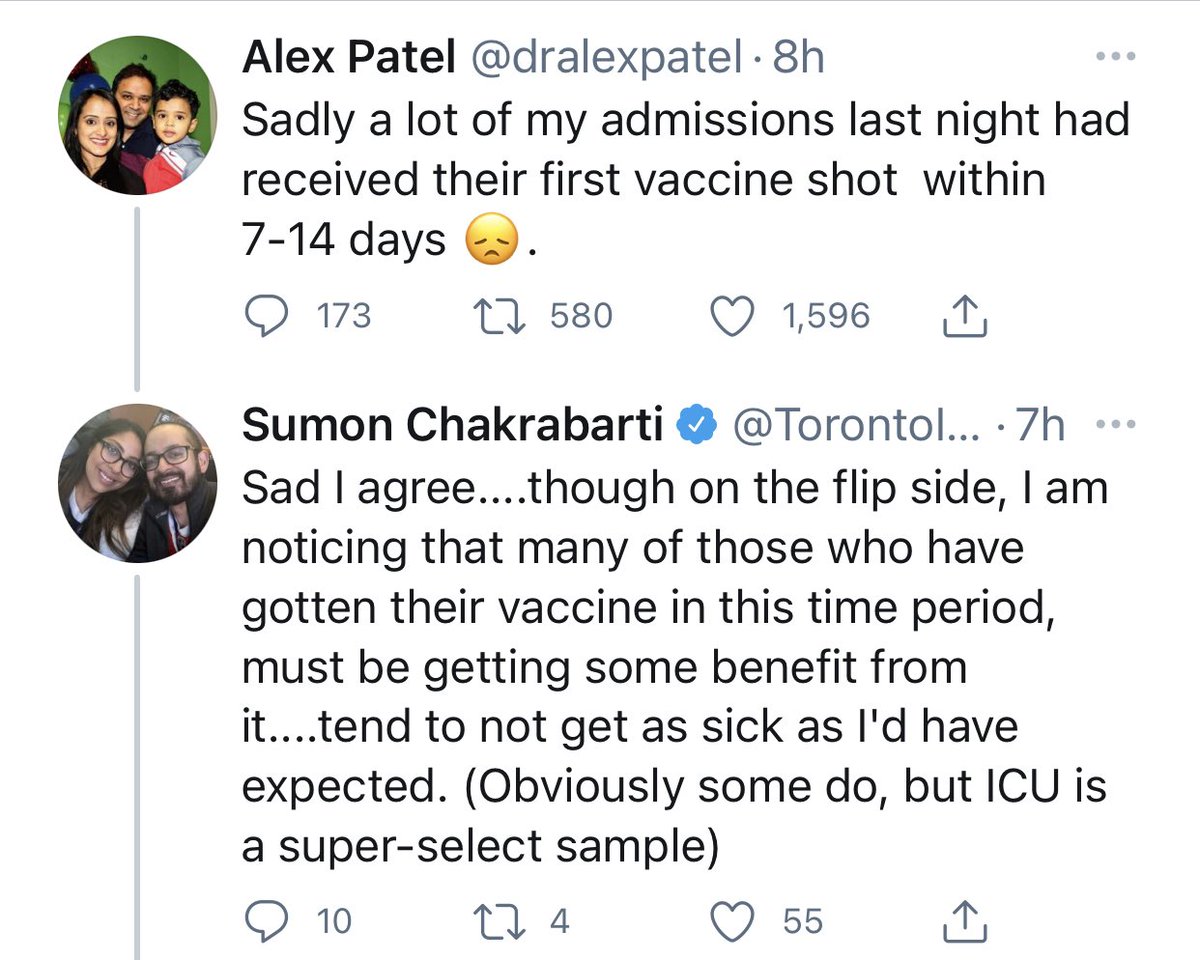
And ICU physicians in Toronto are starting to speak up about vaxxinated people ending up in ICUs as well:
Another important question that needs answering is:
What is the mechanism behind vaxxinated people getting CV19? We unfortunately don’t know yet for sure, but there are a couple of hypotheses being discussed, which I shall address in my next thread soon.






This is worth scrolling as well:
ok folks, grab seat coffee & and have a sit down, because we need to talk about a topic that has been largely ignored by the news media & public health pundits. The seasonality of respiratory viruses
...
4/ Here is how #influenza & coronaviruses cycle throughout the year in #Ontario. You can see the exact same trend; their levels are lowest May-Oct & peak in Jan. Data is for 2013-2020
...

More at link:
https://twitter.com/Metabo_PhD/status/1 ... 27877?s=20
Interpret the above as you deem fit.