Moderators: Elvis, DrVolin, Jeff

![]() by Karmamatterz » Mon Aug 30, 2021 11:23 am
by Karmamatterz » Mon Aug 30, 2021 11:23 am


![]() by Belligerent Savant » Mon Aug 30, 2021 12:13 pm
by Belligerent Savant » Mon Aug 30, 2021 12:13 pm
Iamwhomiam » Sun Aug 29, 2021 8:54 pm wrote:
The fear you few have been in a panic about seems to me to only appear here and nowhere else in my world. And that is usually shared by, bless his heart, bs.
@skye_daddy
·
Look at all those right wing extremists- wait, wait…it’s a mixed group of people standing up against medical tyranny in NY.
Libs of Tik Tok
@libsoftiktok
Thread: Protests against vaccine mandates/passports are happening all across the world.
Thread on all the locations
NYC
Hawaii
Las Vegas
Switzerland
Ireland
Berlin
Paris
London
Belgium
Montreal
Australia
Scotland
Greece

![]() by Belligerent Savant » Mon Aug 30, 2021 1:50 pm
by Belligerent Savant » Mon Aug 30, 2021 1:50 pm
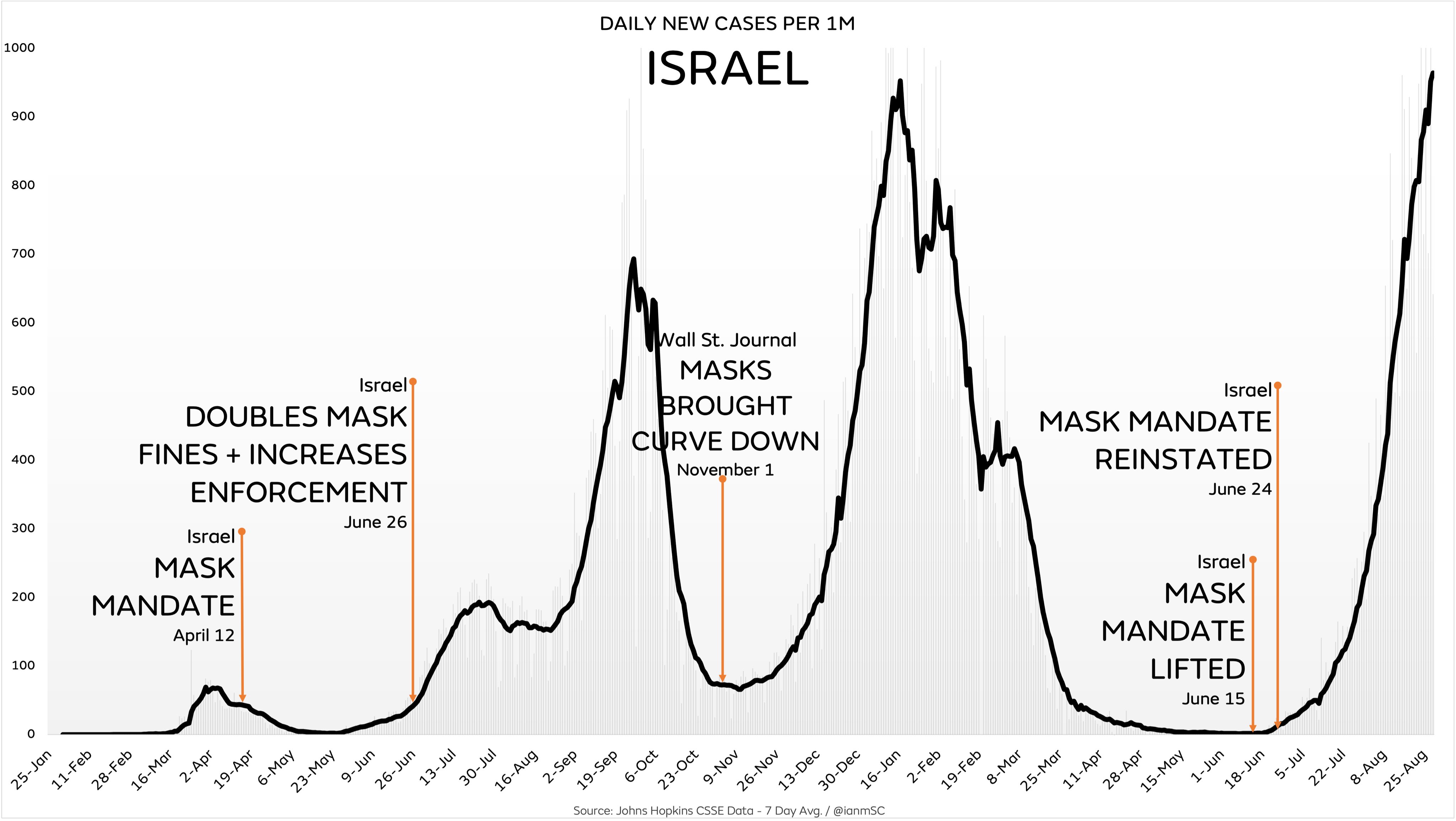
@ianmSC
It’s official, cases in Israel are now the highest they’ve ever been, 2+ months after reinstating their mask mandate
It’s really remarkable to watch experts and the media purposefully ignore reality in order to push for more masking even after it’s already conclusively failed
12:42 PM · Aug 30, 2021
------------------------------------------------------
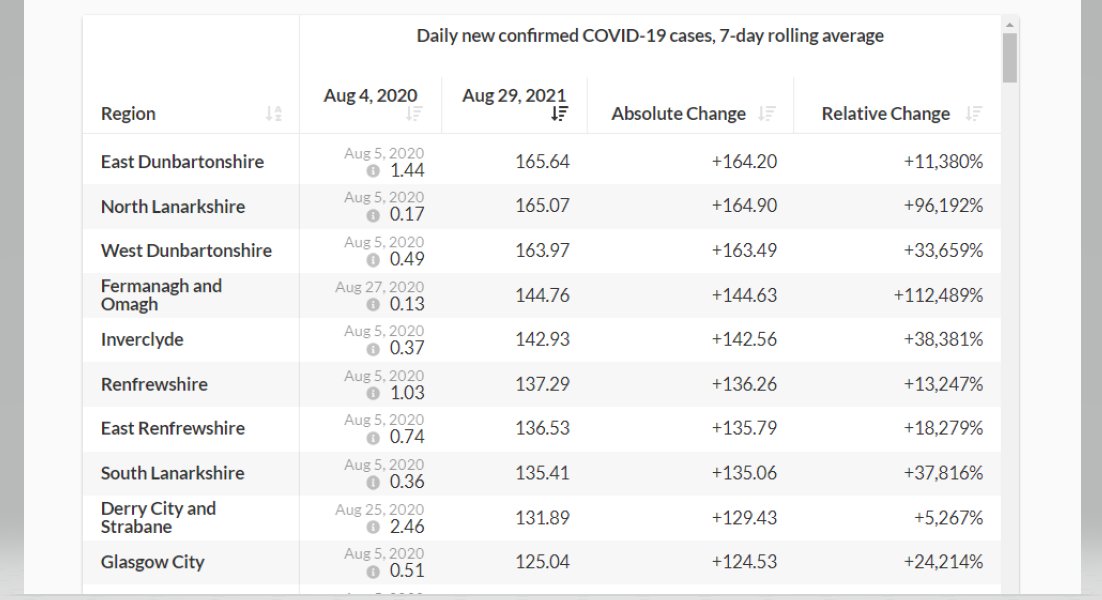
@PaulHainey1
Replying to @ianmSC
Does mass vaccination suppress transmission?
East Dunbartonshire now has the highest case rate in UK: 1,656 per million. (USA peak: 754.2/M, 8th Jan 2021)
Adult (18+) vaccination rates in East D'shire:
2 doses 90.6%
1 dose 98.8%
https://coronavirus.data.gov.uk/details ... artonshire
![]() by DrEvil » Mon Aug 30, 2021 3:28 pm
by DrEvil » Mon Aug 30, 2021 3:28 pm
stickdog99 » Mon Aug 30, 2021 10:23 am wrote:Of course, if our government wanted to do JUST ONE THING to actually stop the spread of COVID-19, it would be to pay people who tested positive for COVID-19 to stay home (or to stay in quarantined COVID-19 care facilities). That clearly should have been the very first mitigating measure.
The bottom line of COVID-19 to me is this.
Any government actually wanting to reduce rates of mortality would have:
* provided free healthcare, especially to suffering from COVID-19 OR any ill health effects from COVID-19 vaccines or treatments
* encouraged healthy lifestyles and provided free nutritious food and nutrition supplements
* protected the vulnerable elderly rather than housing them with infectious patients and euthanizing them with drugs
* set up comfortable places outside of populated areas for infected individuals to voluntarily quarantine
* offered free delivery of life's necessities and a living wage stipend to those who were infected during their quarantine period
* set up a blue ribbon panel of independent medical researchers and clinicians to explore the efficacy of off label drugs for prophylactic and/or remedial treatment for COVID-19 and then deeply examine those showing the most early promise.
Instead, we in the USA have seen a nothing but a singular drumbeat for lockdowns, masks, and experimental vaccines, none of which have yet been scientifically proven to help us more than than they hurt us, but all of which cost the top 0.1% nothing and all of which actually serve to funnel countless billions from the bottom 99.9% to the top 0.1%.
And now, the same top 0.1% is using your irrational fear of COVID and well-fomented hatred of idiot Trumpers to get you to welcome (and even demand) a Big Tech, Big Pharma, and Big Brother dystopia of total bio-security awareness. Wake the fuck up!

![]() by Belligerent Savant » Mon Aug 30, 2021 5:25 pm
by Belligerent Savant » Mon Aug 30, 2021 5:25 pm
This Has Gotta Stop
Lyrics – Eric Clapton
This has gotta stop
Enough is enough
I can’t take this BS any longer
It’s gone far enough
If you wanna claim my soul
You’ll have to come and break down this door
I knew that something was going on wrong
When you started laying down the law
I can’t move my hands
I break out in sweat
I wanna cry
Can’t take it anymore
This has gotta stop
Enough is enough
I can’t take this BS any longer
It’s gone far enough
If you wanna claim my soul
You’ll have to come and break down this door
I’ve been around
Long long time
Seen it all
And I’m used to being free
I know who I am
Try to do what’s right
So lock me up and throw away the key
This has gotta stop
Enough is enough
I can’t take this BS any longer
It’s gone far enough
If you wanna claim my soul
You’ll have to come and break down this door
Thinkin’ of my kids
What’s left for them
And then what’s coming down the road
The light in the tunnel
Could be the southbound train
Lord, please help them with their load
This has gotta stop
Enough is enough
I can’t take this BS any longer
It’s gone far enough
If you wanna claim my soul
You’ll have to come and break down this door
This has gotta stop
Enough is enough
I can’t take this BS any longer
It’s gone far enough
If you wanna claim my soul
You’ll have to come and break down this door
![]() by Belligerent Savant » Mon Aug 30, 2021 7:08 pm
by Belligerent Savant » Mon Aug 30, 2021 7:08 pm
@RWMaloneMD
I don't know quite how to respond. Why is she still in this job? A third jab, with attendant risks, and no data to justify it? We are now officially just winging it, folks. It has come down to this.@JeffereyJaxen
· Aug 24
WH wants boosters for all adults on Sept 20 because of Delta variant...CDC has hope, no data.
---------------------------------
R. Lamartiniere, MD
@rlamartini
·
Aug 26
Replying to @JeffereyJaxen and @NathanNadeson
I was banned from Twitter for a week for questioning the lack of data to support boosters and the reasons behind decisions without data.
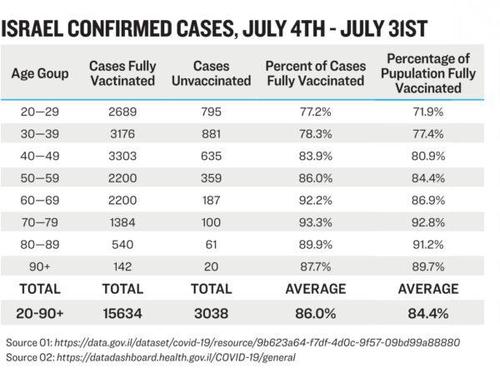
@AanelVictoria
Replying to @RWMaloneMD
People are dropping like flies from the third jab in Israel, which instituted them on July 30:
![]() by stickdog99 » Mon Aug 30, 2021 9:19 pm
by stickdog99 » Mon Aug 30, 2021 9:19 pm
![]() by Harvey » Mon Aug 30, 2021 9:45 pm
by Harvey » Mon Aug 30, 2021 9:45 pm
Their beef is with anything that works.

![]() by liminalOyster » Tue Aug 31, 2021 5:29 pm
by liminalOyster » Tue Aug 31, 2021 5:29 pm

![]() by Harvey » Wed Sep 01, 2021 9:27 am
by Harvey » Wed Sep 01, 2021 9:27 am
The following Notice of Intended Private Criminal Prosecution for mass murder by UK Government policy is an amended version of the notice served upon the Secretary of State for the Department of Health and Social Care last week, which will also be served by email and registered post.
![]() by drstrangelove » Wed Sep 01, 2021 7:37 pm
by drstrangelove » Wed Sep 01, 2021 7:37 pm
TOKYO, Sept 1 (Reuters) - Moderna Inc (MRNA.O) and Takeda Pharmaceutical Co Ltd (4502.T) on Wednesday said they are working with Japanese authorities to recall three batches of COVID-19 vaccine after an investigation found stainless steel contaminants in some vials.
Japanese authorities had suspended use of these batches of Moderna shots containing 1.63 million doses last week after being notified of the contamination issue.
Japan's health ministry said on Wednesday, based on information from the companies' investigation, that it did not believe the particles of stainless steel pose any additional health risk. Moderna said the stainless steel contamination probably occurred during production.
![]() by Belligerent Savant » Wed Sep 01, 2021 9:18 pm
by Belligerent Savant » Wed Sep 01, 2021 9:18 pm
Latest IFR measures
Infection fatality rate
0-19: 0.0027%
20-29: 0.014%
30-39: 0.031%
40-49: 0.082%
50-59: 0.27%
60-69: 0.59%
70+: 5.5%
70+: 2.4% among non-institutional
Who’s Really Being Hospitalized?
Breakthrough cases reach majority levels in some jurisdictions but numbers elude CDC
“I’m not going to arm wrestle with the administration about where to put you,” Dr. C., a highly skilled gastroenterologist, said gently to my friend who was in bed in a triage room in the ER. “We just want to get you into a bed so we can figure out what’s wrong and get you treated.”
We were at our small town’s hospital. No one was sure why, but my friend had not been able to keep anything more than a handful of raspberries down since a complicated surgery for a chronic health condition three weeks before. Dehydrated and unable to eat, my friend had been violently vomiting after taking just a sip of water or sucking on an ice chip, and had lost nearly twenty-five pounds.
I was by my husband’s side when he had a gallbladder attack so severe that it left his hands shaking. I’ve had three unmedicated childbirths and attended many more, both as a journalist and a patient advocate. Still, I’ve never seen a human in so much pain.
Diagnosed with a Pancreas Disorder, Admitted as a COVID Patient
After a battery of testing, my friend was diagnosed with pancreatitis. But it was easier for the hospital bureaucracy to register the admission as a COVID case.
Let me explain. This patient had none of the classic symptoms of COVID: No shortness of breath, no fever, no chills, no congestion, no loss of sense of smell or taste, no neurological issues. The only COVID symptoms my friend had were nausea and fatigue, which could also be explained by the surgery. However, nearly three weeks earlier, a COVID test had come back positive.
The mainstream media is reporting that severe COVID cases are mainly among unvaccinated people. An Associated Press headline from June 29 reads: “Nearly all COVID deaths in US are now among unvaccinated.” Another, from the same date: “Vast majority of ICU patients with COVID-19 are unvaccinated, ABC News survey finds.”
Is that what’s really going on? It’s certainly not the case in Israel, the first country to fully vaccinate a majority of its citizens against the virus. Now it has one of the highest daily infection rates and the majority of people catching the virus (77 percent to 83 percent, depending on age) are already vaccinated, according to data collected by the Israeli government.
After carefully reviewing the available data, including the safety and efficacy profiles of the mRNA vaccines, my friend had taken a cautious approach. Though a medical doctor who gives vaccines in the office every day, my friend opted to wait and see. According to WebMD, a “huge number” of frontline hospital workers have also chosen not to get the vaccine. Indeed, various news reports, from California to New York, confirm that up to 40 percent of health care workers have decided the risks of the vaccines do not outweigh the benefits.
After admission, I spoke to the nurse on the COVID ward. She was suited up in a plastic yellow disposable gown, teal gloves, and two masks underneath a recirculating personal respiratory system that buzzed so loudly she could barely hear. The nurse told me that she had gotten both vaccines but she was feeling worried: “Two thirds of my patients are fully vaccinated,” she said.
Data Limitations
How can there be such a disconnect between what the COVID ward nurse told me and the mainstream media reports? For one thing, it is very hard to get any kind of accuracy when it comes to actual numbers. In fact, the Centers for Disease Control and Prevention (CDC) have publicly acknowledged that they do not have accurate data.
As reported by the Associated Press, “The CDC itself has not estimated what percentage of hospitalizations and deaths are in fully vaccinated people, citing limitations in the data.”
At the same time, data collection is done on a state by state basis. In most states, a person is only considered fully vaccinated fourteen days after they have had the full series of the vaccine.
This means that anyone coming into an American hospital who has only had one dose, or who has had both vaccines but had the second one less than two weeks prior, will likely be counted as “unvaccinated.”
So when the South Carolina’s Department of Health and Environmental Control released a report about COVID severity on July 23, 2021, they reported higher morbidity and mortality rates in the “not fully vaccinated.” Are these people who have had one vaccine and gotten sick, two vaccines and gotten sick, or no vaccines at all? Without more details, it is impossible to know what is really going on.
“We don’t have accurate numbers,” insists Dr. James Neuenschwander, an expert on vaccine safety based in Ann Arbor, Michigan.
But what we do know, Neuenschwander says, is that the vaccines are not as effective as public health officials told us they would be. “This is a product that’s not doing what it’s supposed to do. It’s supposed to stop transmission of this virus and it’s not doing that.”
Overcounting COVID
Then there is the problem of attributing severe illness and deaths from other causes to COVID, like in my friend’s case. Health authorities around the world have been doing this since the beginning of the COVID crisis. For example, a young man in Orange County, Florida who died in a motorcycle crash last summer was originally considered a COVID death by state health officials (after Fox News investigation the classification was changed.) And a middle-aged construction worker fell off a ladder in Croatia and was also counted as a death from COVID (whether having COVID played a role in his death is still unclear.)
To muddy the waters further, even people who test negative for COVID are sometimes counted as COVID deaths.
Consider the case of 26-year-old Matthew Irvin, a father of three from Yamhill County, Oregon. As reported by KGW8 News, Irvin went to the ER with stomach pain, nausea, and diarrhea on July 5, 2020. But instead of admitting him to the hospital, the doctors sent him home.
Five days later, on July 10, 2020, Irvin died. Though his COVID test came back negative two days after his death and his family told reporters and public health officials that no one Irvin had been around had any COVID symptoms, the medical examiner allegedly told the family that an autopsy was not necessary, listing his death as a coronavirus case. It took the Oregon Health Authority two and a half months to correct the mistake.
In an even more striking example of overcounting COVID deaths, a nursing home in New Jersey that only has 90 beds was wrongly reported as having 753 deaths from COVID. According to a spokesman, they had fewer than twenty deaths. In other words, the number of deaths was over-reported by 3,700 percent.
Who’s Suffering from Severe COVID, Vaccinated or Unvaccinated?
In countries with the highest numbers of vaccinated individuals, we are also seeing high numbers of infections. Iceland has one of the most vaccinated populations in the world (over 82 percent) and is reporting that 77 percent of new COVID cases are in fully vaccinated Icelanders, according to Ásthildur Knútsdóttir, Director General of the Ministry of Health.
According to news reports, over 85 percent of the Israeli adult population has been vaccinated. But a July report from Israel’s Ministry of Health found that Pfizer’s vaccine is only 39 percent effective. Though Israeli health officials are telling the public that the cases are more mild in vaccinated individuals, this upsurge in COVID cases and deaths is leading Israel’s prime minister to issue new restrictions.
Dr. Peter McCullough, an academic internist and cardiologist in practice in Dallas, Texas, says that a large number of people in the hospitals right now have, indeed, been fully vaccinated. “Fully vaccinated people are being hospitalized, and … 19 percent of them have died,” McCullough says. “This is not a crisis of the unvaccinated. That’s just a talking point. The vaccinated are participating in this.”
Other physicians are seeing the same thing. “In my practice multiple patients who are fully vaccinated have been admitted to local hospitals,” says Dr. Jeffrey I. Barke, a board-certified primary care physician based in Newport Beach, California. Barke believes part of the problem is exaggeration of the efficacy: “If the vaccine works so well, why are we now pushing a booster?”
Jennifer Margulis, Ph.D., is an award-winning journalist and author of Your Baby, Your Way: Taking Charge of Your Pregnancy, Childbirth, and Parenting Decisions for a Happier, Healthier Family. A Fulbright awardee and mother of four, she has worked on a child survival campaign in West Africa, advocated for an end to child slavery in Pakistan on prime-time TV in France, and taught post-colonial literature to non-traditional students in inner-city Atlanta. Learn more about her at JenniferMargulis.net
Fourth Case Of Contaminated Moderna Vaccine Reported In Japan
Yet another contaminated Moderna Covid-19 vaccine has been reported in Japan - the fourth in less than a week, according to Reuters, which reports that 'several black particles' were found in a Moderna vaccine vial in Kanagawa prefecture.
Last week Japan suspended the use of 1.63 million Moderna doses after being notified of a contaminant which 'could be metal' and reacts to magnets.
Moderna and Spanish pharma company Rovi, which bottles the vaccines, says the cause could be a manufacturing issue.
Kanagawa prefecture said the vaccine's domestic distributor, Takeda Pharmaceutical Co Ltd, had collected the vial with the suspected contaminant and that about 3,790 people had already received shots from the same lot.
. -ReutersMore Moderna shots were temporarily halted in two other regions this week. In some cases, foreign substances have been found in unused vials, whereas others appear to be caused when bits of the vials' rubber stopper break off when needles are incorrectly inserted
On Wednesday, Japan's health ministry said that the vial sent to Kanagawa was from a different lot than the previous contamination reports, but has said that 'rubber stopper material' appears to have gone into it during the manufacturing process (which would contradict last week's report that the material 'reacts to magnets').
Medical staff are being encouraged to perform visual inspections of vials for foreign materials or discoloration before use.
![]() by Belligerent Savant » Wed Sep 01, 2021 10:15 pm
by Belligerent Savant » Wed Sep 01, 2021 10:15 pm
Harvey » Wed Sep 01, 2021 8:27 am wrote:The same Bernician who recently joined RI? If so, good luck with the case. It's the only argument I've heard which does not ignore the UK data from last year and which actually has an evidenced explanation for it: https://www.thebernician.net/notice-of- ... nt-policy/The following Notice of Intended Private Criminal Prosecution for mass murder by UK Government policy is an amended version of the notice served upon the Secretary of State for the Department of Health and Social Care last week, which will also be served by email and registered post.
NOTICE OF INTENDED PRIVATE CRIMINAL PROSECUTION
MASS MURDER BY GOVERNMENT POLICY
According to the World Health Organisation (WHO), “Coronavirus disease (COVID-19) is an infectious disease caused by a newly discovered coronavirus”. However, the genome sequence for SARS-COV-2, released in January 2020, proved that the test to identify its presence was created in the absence of virus samples1. We therefore contend that no virus isolate of SARS COV 2 exists, and that a disease called Covid 19 has not caused excess deaths in the UK.
Our assertion is supported by public documents confirming that no pure isolate of the virus exists2. Furthermore, publicly available death data proves that the so called “first wave of COVID”, and excess deaths in England, only occurred ONCE the pandemic was announced and lockdowns commenced on 23/03/2020, and that a “virus” which was not a HCID, may have been in circulation as early as October 2019.3
On 3rd March 2020, the UK Government scientific advisor echoed the Prime Minister, when he said: “Let me be absolutely clear that for the overwhelming majority of people who contract the “virus”, this will be a mild disease from which they will speedily and fully recover as we’ve already seen”. In line with this, on 13/03/2020, the threat from the virus was officially downgraded from a HCID to a NOID by the Advisory Committee on Dangerous Pathogens [ACDP].4.
However, this decision to downgrade from HCID to NOID was highly controversial because of the WHO’s declaration of a worldwide High Consequence Infectious Disease [HCID] two days previously on 11/03/2020, upon the advice of Neil Ferguson of Imperial College. In other words, the downgrading is an implicit contradiction of Ferguson’s triggering of a worldwide health emergency.
Remarkably, following the private announcement of the downgrading on 13th March 2020, and the subsequent public announcement of the downgrading on 19/03/2020, there appears to have been a premeditated decision to use this unproven ‘pandemic’ as justification to impose measures and medication which went on to kill people. This was in turn used to justify the lockdown measures, which themselves were one of the driving forces of the deaths they claimed to be trying to avoid. This premeditation to cause deaths of course amounts to mass murder by government policy.
There is support for this argument when we look at government policy decisions, which simply put, make no sense. On 17/03/2020, 4 days after the private downgrading mentioned above, the NHS wrote to all hospitals asking them to free-up the maximum possible number of beds by urgently discharging any patients they could.1
Many of these patients were discharged to care homes, some of which were given ultimatums forcing them to take more patients than they were equipped to provide care for. In addition, the NHS cancelled all ‘non-urgent’ treatments.
Why was this policy invented at all given scientific advice on 03/03/2020, and why was it not reversed, given the downgrading on 13/03/2020 by the Advisory Committee on Dangerous Pathogens?
It is our contention that the excess deaths in the first wave occurred AS A RESULT of the relentless implementation of this policy, which was coupled with the inappropriate use of respiratory depressing medications such as Midazolam during the same period. This is how the excess deaths occurred. They were NOT because of a novel virus, isolation of which, according to long held standards, has never occurred.
Our extrapolated data on community Midazolam prescribing supports the above allegation, along with the data on how and where deaths during this time period occurred.
Following the letter of 17/03/2020 from the NHS, bed occupancy in England reduced from the usual 90% to an average of 63% in the spring quarter of 2020. In addition, there was no influx of ‘large numbers of inpatients requiring respiratory support’. Accident and emergency (A&E) departments saw a huge decrease in attendances and overall admitted patient care decreased significantly during the same period.
Of those patients who were admitted to hospital and residents who were discharged to care homes, the outcomes can only be described as devastating. We assert that those outcomes were engineered. When we look at mortality, figures show that hospital and care home death ratios increased during the “first wave” lockdown period2.
Shockingly, 91% of “with COVID” deaths during the first lockdown were of people with any sort of disability3. It is impossible for a ‘virus’ to discriminate in such a manner, and therefore we contend these deaths must have been as a result of very nefarious policies. These policies were blanket DNRs and mandatory prescribed medications, two factors which have contributed to most other “non disability” deaths during the first lockdown period.
Data proves that up to 13/05/2020, deaths in care homes from all causes were 159% higher than at the start of “the COVID-19 outbreak”4. In April 2020, the ratio of excess deaths in English care homes was almost three times that of the prior five years’ average. It is not a mere coincidence that during the same month, prescribing of Midazolam increased by more than 100%5. There is a clear correlation between policy, prescribing of Midazolam and deaths, which simply cannot be overlooked.
Further,more during the period 2 March to 12 June 2020, 18,562 residents of care homes in England died, supposedly “with COVID-19”, including 18,168 people aged 65 and over. This represented almost 40% of all deaths involving “COVID-19” in England during this period 6
In addition to the above, during the first lockdown there was an unbelievable policy change in care homes7. The change restricted access for residents’ families. This removed crucial oversight of treatment along with safeguards. Also, support services such as SALT, chiropody, physiotherapy and in house GP visits, were removed.
Simply put, care homes were turned into death camps and their inmates were targeted for elimination. Staffing levels dropped due to a policy of self-isolation for anything akin to a sniffle, and this further pressured care homes who then had a ratio of staff to patients that was unworkable.
We contend this was not an accident, and instead was done by design. Only a fool, or perhaps a madman, would implement such policies and not realise the inevitable consequences. Only a fool or a madman would say they were necessary after the down grading of Covid 19 from an HCID to a NOID on 13/03/2020.
As we have already stated, we assert that the above were premeditated policies, to cause excess deaths in care homes (as well as in the community generally). It is without doubt that family surveillance in care homes, at a time when staff limits were stretched, could have stopped avoidable deaths. Furthermore, had support services been available, we very much doubt that the over prescribing of respiratory depressing medication would have been either necessary, or allowed to transpire.
Bizarrely, in addition to the above, all official inspections were suspended during the first lockdown, leading to less and less oversight. Very worryingly, the use of blanket DNRs,8 (now acknowledged as a fact by Matt Hancock), as well as do not admit to hospital orders, were imposed, and undoubtedly led to countless avoidable deaths.
Lockdown restrictions eased at the start of June 2020 and up to the start of the second national lockdown, there was NEGATIVE excess deaths in care homes (a ratio of 0.96 versus expected levels). This fall in deaths occurred in the absence of any ‘vaccines’ or alternative treatment for so called Covid 19.
We therefore contend that the initial wave of deaths during the first lockdown were driven by policy decisions by this government and Midazolam prescribing. These deaths were in fact accelerated deaths, rather than excess deaths, and these accelerated deaths were created for political and policy gain, to feed a narrative of a deadly pandemic which simply did not, and still does not, exist.
Jay Bhattacharya, a Stanford professor, has labelled lockdowns “the single biggest public health mistake in history”9. 95% of hospital COVID-labelled deaths occurred DURING lockdown. How is this possible if lockdowns save lives?
We contend that lockdowns kill, but moreover that they are designed to do so. However, lockdowns alone do not provide the significant number of deaths needed to create the illusion of a pandemic. This is the primary reason we have looked at Midazolam prescribing during this period.
It is a well-known fact that Midazolam is a respiratory depressing drug1. It creates the very respiratory symptoms of so called “COVID-19”. Used in copious amounts in conjunction with lockdowns, Midazolam led to premature deaths. The data we have extrapolated on community Midazolam prescribing supports this, along with the pertinent observations above, about where and how accelerated deaths occurred.
Given our assertions that government policy and Midazolam prescribing have caused accelerated deaths, and our assertion that this was designed and premeditated by certain individuals within and advising this government, we have some questions that we wish to put to you.
Our allegations described above are of the most serious kind. In the absence of satisfactory answers from you to our questions and given the supporting evidence we are presenting with this notice, we wish to make clear that we will assume you cannot prove beyond reasonable doubt, that what we have asserted about a government premeditated policy of mass murder is false.
Let us be clear, this is your chance to answer the questions posed and give proof that our allegations and assertions are wrong. If you can do that by bringing evidence to the contrary of ours, we will accept that we have perhaps misinterpreted our evidence, albeit in good faith.
However, you will need to produce sufficient material evidence to rebut our allegations, and in the absence of the same, we will pursue a Private Criminal Prosecution based on the statements made herein.
Of the 50,335 deaths which occurred in March to June 2020 involving COVID-19 in England and Wales, 45,859 (91.1%) had at least one pre-existing condition, while 4,476 (8.9%) had none. It is for those people and their families that we so urgently seek a just outcome in this the most serious type of criminal proceedings imaginable.
Questions About Allegedly Murderous UK Government Policy
How much 1mg 5ml Midazolam Hydrochloride ampules were used in England between March and May 2020?
Of 1mg in 5ml Midazolam Hydrochloride ampules used between March and May 2020, where were they prescribed, and in what proportion, i.e. what went into the community, and what went into hospitals?
What was the UK stock of 1mg 5ml Midazolam Hydrochloride ampules held for the months October 2019, November 2019, December 2019, January 2020 and February 2020?
How much 1mg 5ml Midazolam Hydrochloride ampules were left in the UK in October 2020?
What was the UK stock of 10mg 2ml Midazolam in the months October 2019, November 2019, December 2019, January 2020 and February 2020?
How much 10mg 2ml Midazolam Hydrochloride ampules were left in the UK in October 2020?
Who ordered the 22,000 extra packs in May 2020? Was it the DHSC, and if so, which minister signed off the order? If it was not the DHSC please specify who it was?
What was the cost of the order of the 22,000 packs?
Moving on to the Health and Social Care Committee. Oral evidence: Preparations for Coronavirus, HC 36, Friday 17/04/2020, ordered by the House of Commons to be published on 17/04/2020, what does Dr Luke Evans mean when he says, “a good death”?
Does he mean euthanasia, which this term commonly refers to?
Assuming he does mean this, why did Dr Luke Evans openly discuss government policy of causing “a good death” by administering fatal dose of drugs like Midazolam and Morphine, via hypodermic syringes, when to do so is tantamount to an implicit confession of mass murder by policy?
Euthanasia and assisted suicide are both illegal under English Law. Assisted suicide is illegal under the terms of the Suicide Act (1961) and punishable by up to 14 years’ imprisonment. Depending on the circumstances, euthanasia is regarded as either manslaughter or murder.
Are Dr Luke Evans’ remarks a result of the Confidential Pandemic Influenza (CPI) briefing paper dated 08/09/2017, which states, and we quote: “There is significant discussion in the paper about ceasing or changing care to patients in the HRG categories; however a decision may more appropriately be taken to treat patients in the listed HRG groups rather than influenza patients, dependent upon likelihood of survival……… Total excess death rate would be in excess of 7,806 per week of the peak of the pandemic if all these services were stopped. So, in the peak six weeks of a pandemic (recognising the typical profile of increasing and decreasing case numbers either side of the peak weeks), 46,836 excess deaths could be expected. On the one hand, this is likely to be an underestimate as it only considers the top 14 HRG codes and it does not consider additional deaths occurring particularly in the elderly and frail across primary care where HRGs are not coded.”
Give the CPI and Dr Luke Evans’ remarks, is there a culture within government, Public Health England and indeed the NHS to enact the supposedly defunct Liverpool Care Pathway, to end lives at the behest of the treating doctor, which of course is illegal as described above?
If the answer is “no”, can you please explain why the NHS drew up the CPI and included within it plans to withdraw hospital care from people in nursing homes in the event of a pandemic, which also included refusal to treat those in their 70s and instead offer “support” to use so-called “end of life pathways”.
The CPI states that the Health Secretary (at the time) could authorize medics to prioritize some patients over others and even stop providing critical care altogether. Was such a decision taken by the Health Secretary at the time, (Matt Hancock), in relation to care home, hospital and community residents over a certain age?
Government ministers have repeatedly insisted that care homes were not abandoned by the NHS during the coronavirus crisis, despite more than 42,000 residents in England and Wales dying during the “pandemic”. Given this, what is your proof that this was not because of decisions made by the DHSC, and/or PHE and NHS chiefs, which then resulted in thousands of needless deaths?
Care homes were asked by NHS managers and GPs to place DNR’s on all residents at the height of the “pandemic” to keep hospital beds free – in breach of guideline 3. Blanket DNR’s were also imposed on people with learning disabilities “who were not near the end of their lives”, showing a concerning disregard for disabled people. Who made the decision to ask care homes to do this, and were these decisions taken because of the CPI?
In making his remarks at the Health and Social Care Committee, Oral evidence: Preparations for Coronavirus, HC 36, Friday 17 April 2020, why did Dr Evans and indeed all those present, completely ignore the declassification of COVID-19 from an HCID to a NOID on 13/03/2020, meaning that such nefarious measures as those mentioned in the CPI were never necessary?
Moving on, we attach a selection of graphs regarding the prescribing of 10mg 2ml Midazolam hydrochloride ampules for various years and months. Can you please explain why the enormous increase in Midazolam prescriptions for 10mg 2ml Midazolam hydrochloride ampules coincide with implementation of the UK Government’s COVID-19 Battle-plan in March 2020?
How much 10mg 2ml Midazolam hydrochloride ampules, were held in the UK in January 2020, and what wholesalers held them? How does the DHSC, PHE and the NHS keep track of what stock it has of 10mg 2ml Midazolam hydrochloride ampules, and indeed all other Midazolam products?

Users browsing this forum: No registered users and 6 guests
Powered by phpBB® Forum Software © phpBB Group
Site design by Likely Arts based on "Deluxe" by Artodia.