Lethal Infection of Human ACE2-Transgenic Mice Caused by SARS-CoV-2- related Pangolin Coronavirus GX_P2V(short_3UTR)
4th January 2024
New brain virus

Just kidding, He's not a doctor....
Moderators: Elvis, DrVolin, Jeff
![]() by Grizzly » Fri Jan 12, 2024 1:11 am
by Grizzly » Fri Jan 12, 2024 1:11 am

![]() by Grizzly » Fri Jan 12, 2024 7:59 pm
by Grizzly » Fri Jan 12, 2024 7:59 pm
![]() by Grizzly » Sun Jan 14, 2024 12:48 am
by Grizzly » Sun Jan 14, 2024 12:48 am
![]() by Grizzly » Sun Jan 14, 2024 3:18 pm
by Grizzly » Sun Jan 14, 2024 3:18 pm
7:19
yet but we do know it's out there uh do
7:23
we but we do know it's out there now
7:26
unfortunately much to my annoyance and
7:29
your annoyance I
7:31
felt um compelled to delete yesterday's
7:35
um video my apologies the the the trick
7:39
is to live to fight another day um
7:42
that's what we aim for but the video I
7:45
was doing yesterday was examining a
7:47
particular virus uh that was uh
7:50
experimentally used to infect mice
7:53
caused a disease of the brain and on at
7:56
the end of the study none of the mice at
7:59
the end of of the study were alive
8:00
anymore none of them were alive
8:03
anymore um because a certain event had
8:05
happened to them that made them not
8:09
alive um and that virus my understanding
8:13
from reading of the paper was it had
8:16
been it evolved in cell cultures in a
8:22
laboratory so as a result of going
8:25
through cell coaches in a laboratory the
8:27
function of the virus had been uh had
8:30
been increased it would appear it became
8:33
a more functional virus there was a
8:38
function and uh there was potentially um
8:43
an
8:44
increase uh maybe even a
8:47
gain uh anyway but but um we know it's
8:51
out there so they know it's out there
8:55
uh obviously they don't know a precise
8:58
geographical location but they know it's
9:00
out there uh and we know it has the
9:02
potential to spill over from animal
9:05
populations potentially into humans well
9:08
yeah there can be natural spill over
9:09
vents of course there can also be other
9:12
origins of viruses perhaps mutate or
9:15
adapt itself and then begin spreading
9:16
and killing people faster than we can
9:19
contain
9:20
it um carrying out research and oh and
9:24
vaccine development carrying out
9:25
research and vaccine
9:27
development for no own viral families
9:31
could impact humans of which there are
9:33
25 viral families they're saying uh
9:37
would give Humanity a decided advantage
9:39
over the next disease
9:42
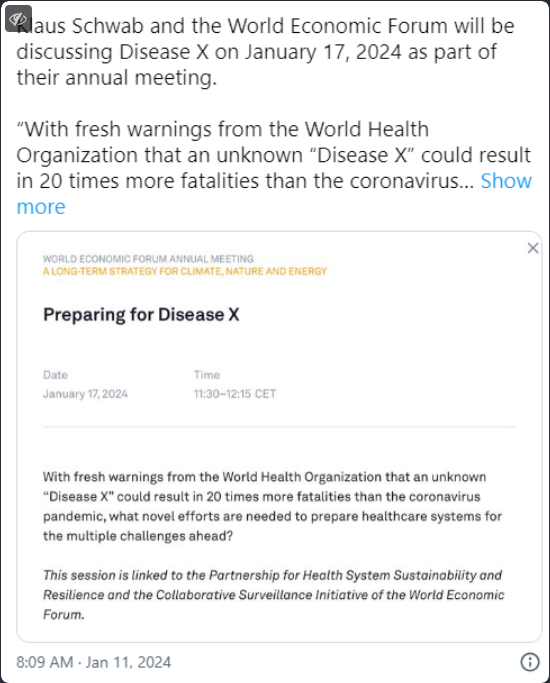
X so who who knows maybe the world
9:45
economic Forum will be good enough to uh
9:48
develop a vaccine for as great unwashed
9:50
so it's all ready for us
hello warm welcome to this talk Saturday
0:03
the 13th of January now I want to be
0:05
talking about disease X in a minute from
0:08
a small radio station in Switzerland
0:10
called radio Davos I think it was more
0:13
on that shortly but a bit of a
0:15
disappointment first this is from the UK
0:20
Co inquiry and unfortunately the uh
0:23
public hearings for the inquiry fourth
0:27
investigation into vaccines and
0:29
therapeutic module will be
0:32
rescheduled the hearings were
0:33
provisionally scheduled to take place in
0:35
the summer of 2024 they will now take
0:38
place at a later date and then there's
0:42
some rationale given there which you may
0:45
choose to accept or not to enable
0:47
organizations to prioritize providing
0:49
evidence for the inquirer's third
0:51
investigation into the impact of the
0:53
pandemic on healthare well I would have
0:55
thought um they knew what order this was
0:58
in before they did this but never mind
1:01
that's what they've said this is from
1:03
the site here um this is from baroness
1:07
Hallet who's the chair of the inquiry I
1:09
know that the postponement of these
1:11
hearings will be a disappointment for
1:12
some yes it will and I think there's a
1:15
degree of urgency as I'll point out um I
1:18
want to ensure our hearings of uh in
1:20
2024 are as effective as possible well
1:24
yes and I recognize the increasing
1:26
pressure on organizations to respond to
1:28
requests and provide information to the
1:29
inquiry now I would have thought they'd
1:31
known that when they scheduled the
1:34
inquiry at the first place um maybe um
1:38
they've had to reschedule this because
1:39
there was some new information came to
1:42
light we we we're basically not told
1:45
which is
1:46
disappointing but we are assured it's
1:48
going to be finished by the summer of
1:50
2026 so let's hope there is time to
1:53
squeeze in this rather important module
1:57
because it's not on as scheduled
2:00
unfortunately so I had been genuinely
2:03
looking forward to that and it's pretty
2:04
disappointing that that is now being
2:06
delayed now I want to give you something
2:08
from the mail online now that I'm just
2:10
hoping they don't know more than we do
2:12
about it because they actually say uh Co
2:15
inquirers probing to vaccines is delayed
2:17
indefinitely indefinitely they're saying
2:21
well let's hope that's not the case uh
2:23
as chair admits postponement will be a
2:25
disappointment for some yes um hearing
2:28
for the fourth module of this is from
2:29
the from the mail online now hearing of
2:31
the fourth module of the official
2:32
inquiry to be what what it was set of
2:35
the official inquiry were set to begin
2:37
this
2:38
summer a long awaited probe into the
2:41
development of covid vaccines and drugs
2:42
was today postponed and again they say
2:45
indefinitely here so let's hope this is
2:47
not the
2:49
case baroness Hallet says I know the
2:51
postponement will be a disappointment I
2:53
wish to reassure you that we will hold
2:55
these hearings as soon as possible good
2:58
we'll look out for it uh but we're still
3:00
going to be finished by the summer of
3:02
2026 so let's hope it's time now this
3:05
inquiry has cost you and me the plait
3:07
Ariat the pans so far it's cost us 145
3:11
million
3:13
um quite incredible now um I'm going to
3:16
talk about disease X in a minute but
3:18
just before we do that um this is just a
3:21
completely unrelated uh article I was
3:24
reading in the Guardian newspaper from
3:26
November 2022 this is Paul Burl who was
3:28
a royal Butler and Paul borrow reported
3:32
a conversation with her majesty the
3:33
queen prior to her sad recent uh
3:38
departure uh and Paul Bor reports that
3:41
the queen said this Queen Elizabeth said
3:43
this there are powers at work in this
3:45
country about which we have no knowledge
3:48
so uh it looks like uh there are powers
3:51
at work uh but we don't know what they
3:53
are so in Donald Rumsfeld terms this
3:55
would be a known unknowns I guess now I
3:58
want to talk now about disease
4:01
X which is on this website here this is
4:05
the uh World economic Forum site as far
4:09
as I can uh derive disease X this is how
4:12
we should prepare for the next big
4:15
virus wow so uh this you can listen to
4:18
it here or you can um read it there it's
4:20
all very easy to understand while being
4:25
rather uh difficult to understand now
4:28
disease X
4:30
um I've been teaching this sort of thing
4:32
pretty well fulltime since
4:35
1990 I know I've been a clinical nurse
4:38
since 1975 when I was a first year
4:41
student and um I'd never heard of this
4:43
disease X so I looked at some of my
4:45
books because when I wrote my book I
4:48
couldn't remember putting it in so it
4:50
wasn't in there but I could easily miss
4:53
it couldn't I so I did check in uh
4:55
Reuben's pathology these are the
4:57
definitive texts see it in there
5:01
either uh so I checked in G and Hall
5:04
superb physiology book not in there
5:06
either
5:08
um uh porth's
5:11
pathophysiology um not in there either
5:13
it's fairly thick book you think it
5:15
could be in there somewhere um you get
5:18
the idea not in that one can hardly pick
5:20
this one up path physiology all these
5:23
standard textbooks um not in there so it
5:27
must be a new
5:30
disease can't say I like the sound of a
5:32
new disease we've had a new disease
5:33
already haven't we anyway um this is
5:36
just I want to give you some highlights
5:38
from the um the radio Davos uh talk
5:45
disease X is looming the world needs to
5:48
be better prepared to tackle a future
5:50
pandemic and you'll see here that the
5:53
text is from the world economic Forum
5:56
site um they go on to say
6:00
uh by mapping viruses with the potential
6:03
to become the next disease X the global
6:06
Health Community and
6:08
governments uh the governments and
6:10
governments can be more
6:12
responsive the next time a pandemic
6:16
looms looks like they're anticipating
6:18
another pandemic here Global
6:20
collaboration and adequate funding are
6:22
needed to improve pandemic preparedness
6:23
and ensure fast
6:25
action to keep a viral outbreak at Bay
6:31
uh it says you can get a long way being
6:34
able to produce something not quite sure
6:37
what's being produced but you can
6:38
produce something or other something or
6:41
other that will Target a novel virus
6:44
before that virus even emerges I assume
6:47
here they're referring to repurpose
6:49
drugs which could be rolled out very
6:52
quickly and uh very cheaply and may be
6:55
efficacious against a range of
6:57
conditions maybe that's what they mean
6:59
but anyway they're going to produce
7:02
something um can't read too much into
7:04
that all they say is something could
7:06
even mean a vaccine I don't know
7:07
whatever they mean there um anyway that
7:11
will Target a novel virus before that
7:13
that virus even
7:16
emerges um it's a virus we don't know
7:19
yet but we do know it's out there uh do
7:23
we but we do know it's out there now
7:26
unfortunately much to my annoyance and
7:29
your annoyance I
7:31
felt um compelled to delete yesterday's
7:35
um video my apologies the the the trick
7:39
is to live to fight another day um
7:42
that's what we aim for but the video I
7:45
was doing yesterday was examining a
7:47
particular virus uh that was uh
7:50
experimentally used to infect mice
7:53
caused a disease of the brain and on at
7:56
the end of the study none of the mice at
7:59
the end of of the study were alive
8:00
anymore none of them were alive
8:03
anymore um because a certain event had
8:05
happened to them that made them not
8:09
alive um and that virus my understanding
8:13
from reading of the paper was it had
8:16
been it evolved in cell cultures in a
8:22
laboratory so as a result of going
8:25
through cell coaches in a laboratory the
8:27
function of the virus had been uh had
8:30
been increased it would appear it became
8:33
a more functional virus there was a
8:38
function and uh there was potentially um
8:43
an
8:44
increase uh maybe even a
8:47
gain uh anyway but but um we know it's
8:51
out there so they know it's out there
8:55
uh obviously they don't know a precise
8:58
geographical location but they know it's
9:00
out there uh and we know it has the
9:02
potential to spill over from animal
9:05
populations potentially into humans well
9:08
yeah there can be natural spill over
9:09
vents of course there can also be other
9:12
origins of viruses perhaps mutate or
9:15
adapt itself and then begin spreading
9:16
and killing people faster than we can
9:19
contain
9:20
it um carrying out research and oh and
9:24
vaccine development carrying out
9:25
research and vaccine
9:27
development for no own viral families
9:31
could impact humans of which there are
9:33
25 viral families they're saying uh
9:37
would give Humanity a decided advantage
9:39
over the next disease
9:42
X so who who knows maybe the world
9:45
economic Forum will be good enough to uh
9:48
develop a vaccine for as great unwashed
9:50
so it's all ready for us
9:53
um I'll leave it with you read the
9:56
article for yourself it's all there um
10:02
it's all there yep from Radio
10:10
Davos quite concerning really a disease
10:15
X they seem to think it's
10:21
coming um that's hope they don't know
10:23
too much more than us we'll leave it
10:26
there thank you for watching
![]() by stickdog99 » Wed Jan 17, 2024 10:27 pm
by stickdog99 » Wed Jan 17, 2024 10:27 pm
![]() by Grizzly » Mon Jan 22, 2024 10:25 pm
by Grizzly » Mon Jan 22, 2024 10:25 pm

![]() by Belligerent Savant » Fri Jan 26, 2024 8:55 pm
by Belligerent Savant » Fri Jan 26, 2024 8:55 pm

![]() by stickdog99 » Tue Feb 27, 2024 6:45 pm
by stickdog99 » Tue Feb 27, 2024 6:45 pm
![]() by Belligerent Savant » Wed Feb 28, 2024 12:17 pm
by Belligerent Savant » Wed Feb 28, 2024 12:17 pm
Revisiting China: Did a Pandemic really start in Wuhan?
While there has been much debate about where the virus came from, few have questioned that a pandemic started in Wuhan. We look in more detail at what happened in China in early 2020.
BY THOMAS VERDUYN, BASC
28 FEBRUARY 2024
Nearly four years ago, on 11 March 2020, the World Health Organization (WHO) officially declared that “Covid-19 could be characterised as a pandemic.”[1] The series of events leading up to this remarkable statement began only ten weeks earlier (31 December 2019) when the WHO “picked up media reports of … a cluster of cases of pneumonia of unknown cause in Wuhan.”[1] As a result, it has been taken for granted by most that the city of Wuhan was the starting point of the Covid pandemic. While there has been much debate about where the virus came from—that is, whether it jumped to humans from an animal source at the Wuhan wet market or whether it leaked from the Wuhan Institute of Virology—few have questioned that a pandemic started in Wuhan.[2]
Science, however, is not about taking things for granted, but about questioning narratives and investigating facts. With this in mind, we wish to consider in more detail what happened in China in early 2020.
The City of Wuhan
The city of Wuhan with its population of more than 11 million people is about 20% larger than New York City (NYC), the largest city in the US. It is the capital city of the Chinese province of Hubei, and is considered one of the nine most important cities in China.[3] On 23 January 2020, this enormous city was “placed under lockdown due to the 2019 Novel Coronavirus outbreak.”[4] Hubei and other provinces in China followed suit soon after, albeit with different levels of restrictions.[5, 6]Locking down a province of 58 million people for just 17 deaths in 24 days is certainly an extreme response.
During the 24 days between 31 December 2019 (when something “unknown” was first picked up) and 23 January 2020 (when Wuhan was “locked down”), the total number of cases of Covid in the entire province of Hubei was 444. The number of deaths attributed to Covid during this same 24-day period was seventeen.[JHU CSSE COVID-19 Data,7] Although some people question the validity of Covid data emanating out of China, it is important to note that the WHO accepted the data as reliable, and their decisions were based on it.
It is helpful to put this number of deaths into perspective. The crude mortality rate of Hubei is about 5.9 per 1,000 residents,[8] and the population of Hubei is 58 million. Thus, on average, 22,500 people in Hubei die during a normal 24-day period. The 17 Covid deaths, therefore, were effectively negligible. Locking down a province of 58 million people for just 17 deaths in 24 days is certainly an extreme response.
Was there something particularly lethal about Covid that warranted it? Based on the number of reported cases (444) and deaths (17), the case fatality rate (CFR) of Covid in Hubei province as of 23 January 2020 was 3.8%. For all of China it was 2.6% (17 deaths, 643 cases). Although this is higher than that for influenza A, it is four times less than the CFR of SARS, thirteen times less than that for MERS, and there are several dozen other human infectious diseases with a CFR greater than 2.6%.[9] Also, and more importantly, the CFR for any “unknown” disease will almost certainly appear much higher than it actually is until more information becomes available. Indeed, only one week later (1 February 2020), the CFR had already dropped to 0.7%,[10] and was showing signs of being on par with the flu.
Two days after the city of Wuhan was locked down, the Chinese New Year was ushered in (25 January 2020). This day is an important holiday in China. It usually involves many days of festivities and of increased travelling, making it “the world’s largest annual migration.”[11] Since the surge in travel volumes usually begins two weeks before the New Year, it had been ongoing for some time before the lockdown was initiated. According to Fan et al., “Due to the impending Chinese New Year, more than five million people travelled from Wuhan for either family reunions and/or holidays, contributing to the subsequent outbreak of Covid-19 in every province/region in China within a matter of weeks.”[12] The notion of locking down a province to stop the spread of a virus after five million people had already left the province, and would shortly return, makes this response even more odd.
Covid Cases in China
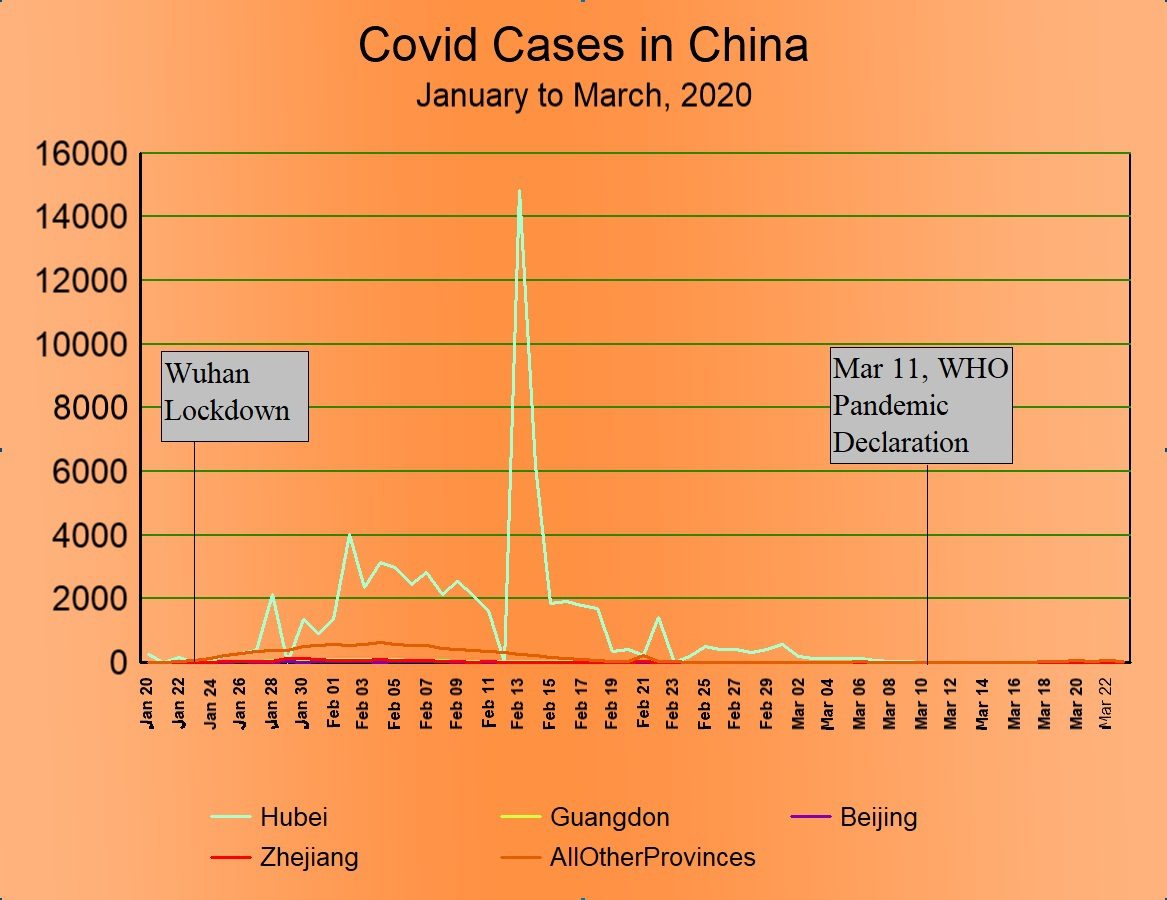
How bad was the “outbreak” of Covid that was purported to have been caused by this mass migration? To answer this question, we plotted Covid cases in China by province from January to March 2020. As case numbers were so small in most provinces, we show only the four provinces with the highest numbers of cases. The remaining 29 provincial regions (Taiwan is excluded) are lumped together and treated as a single entity.
Figure 1: Daily Covid Cases by Province in China, for the four provinces having the largest number of cases. Hubei province (light grey) dominates the graph. The other three provinces included in the graph (Guangdong, Beijing, and Zhejiang) are almost zero the entire time. “AllOtherProvinces” (brown line) is the daily sum of the remaining 29 provincial regions. Source: JHU CSSE COVID-19 Data. https://github.com/CSSEGISandData/COVID-19
Several aspects of the preceding graph are worth noting. In the first place, the number of cases in Wuhan dwarfed all other provinces combined. Total cases in Hubei by the end of March amounted to 67,800, whereas the combined total in the other 32 provincial areas was only 13,639. Therefore, despite the exodus of five million people out of Wuhan in the days leading up to the lockdown, despite there being cases in every other province, and despite the other provinces not being locked down as tightly as Hubei province was, somehow the SARS-CoV-2 virus didn’t seem to spread in those provinces. Nor can the difference be attributed to population density, as 14 of the 33 provincial regions are more densely populated than Hubei.
Second, the spike in cases that occurred in Hubei province on 13 February 2020 is somewhat misleading. The increase resulted because China changed its policy and began including not only lab-confirmed cases but clinically diagnosed cases as well.[13] This policy change was in place for about two weeks and, in consequence, artificially inflated the number of cases by about ten thousand. Covid, after all, is clinically indistinct from other common respiratory viruses.[14]
Third, the total number of cases in China in the first three months was 81,439. Given that China has a population of 1.5 billion, it is observed that during these three months less than 0.006% of the populace was infected. Such a low number of infections argues strongly against the common claim that Covid is a “highly contagious disease.”[15] This is especially so given the fact that this almost negligible infection rate happened in the context of a mass migration and millions of family gatherings.
Fourth, the lockdown of Wuhan and the restrictions placed on the rest of China seem to have had no impact whatsoever on the trajectory of Covid cases. Cases began to rise after the lockdown was initiated, continued along a generally increasing trend for three weeks thereafter, and then tapered off to zero. By the time the WHO declared Covid a pandemic, it had entirely fizzled out in China.
Multiple published studies have claimed that the lockdown of Wuhan successfully eradicated Covid from the province. To justify the claim, the authors typically assume a three-week lag, thereby making the drop in cases artificially align with when the lockdown supposedly began to take effect.[16, 12] However, the papers we looked at have no more proven that the lockdown caused the decline than that the Chinese New Year caused it, for the timing of that event is also about three weeks before cases peaked. Furthermore, multiple studies into the usefulness of lockdowns in other countries concluded that lockdowns did not change the trajectory of Covid.[17, 18, 19] Figure 1 above is a powerful visual demonstration of this.
Covid Deaths in China
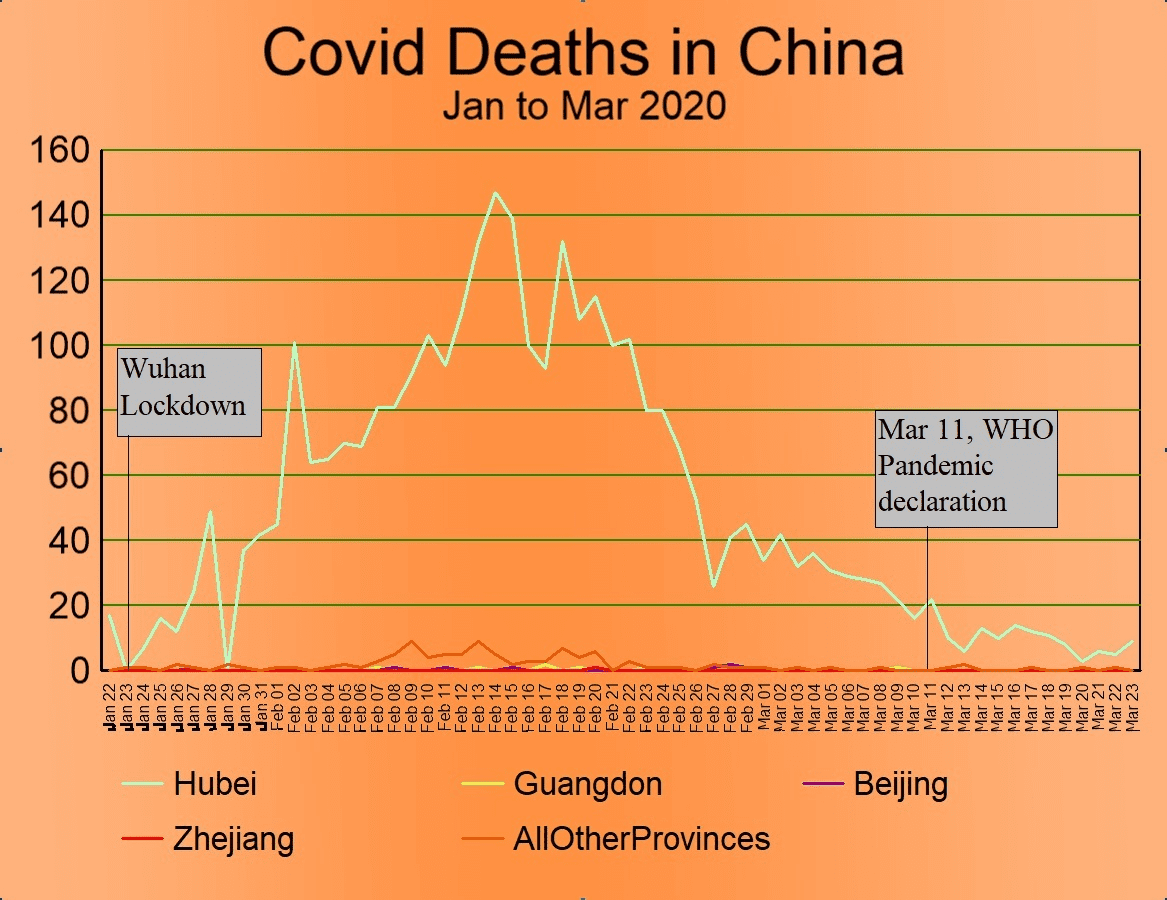
Having considered Covid cases, we turn next to examine the number of deaths attributed to Covid in China. Figure 2 below plots daily Covid deaths in the first three months of 2020. We have used the same provincial strategy as was used above (Figure 1) in the plot of Covid cases.
Figure 2: Daily Covid deaths in China for the four provinces having the largest number of cases. A two-day rolling average was used to smooth out the curve somewhat. Hubei (light grey) is the province that dominates the graph. The brown line labelled “AllOtherProvinces” represents the daily sum of deaths for all the remaining 29 provincial regions. Source: JHU CSSE COVID-19 Data. https://github.com/CSSEGISandData/COVID-19
Once again, several notable observations can be made from this graph. First, the lockdown of Hubei province was initiated when daily deaths were almost zero.
Second, as with cases, the lockdown seems to have had no impact whatsoever on the trajectory of Covid deaths. Deaths generally rise for three weeks after the lockdown, peak on 14 February 2020 (one day after the peak of cases), and then taper off to zero over the next six weeks. By the time the WHO declared Covid a pandemic, deaths attributed to Covid in China were trending rapidly to zero.
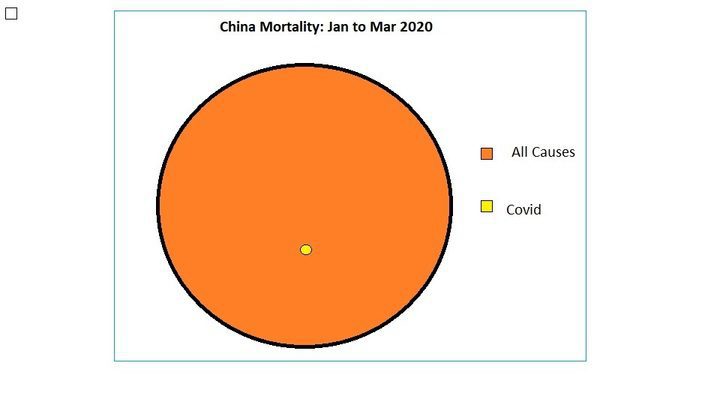
Third, the total number of deaths (3,285) and the peak (152) are extraordinarily small numbers when placed in the context of the enormous Chinese population. By way of comparison, in a typical three-month period, 2.48 million people in China die.[20] We compare these two numbers visually in the following diagram. (See Figure 3).
Figure 3: Cumulative mortality in China from January 1 to March 31, 2020. The orange circle includes all-cause mortality. The small yellow dot represents the relative number of Covid deaths in the same period. All-cause mortality is based on the crude mortality rate in China. Source of Covid deaths is from JHU CSSE COVID-19 Data. https://github.com/CSSEGISandData/COVID-19
Conclusion
Having examined the data regarding Covid cases and deaths in China in the first three months of 2020, we observed that the lockdown of Hubei province was followed by a very slight surge in Covid cases and deaths. Both had fizzled out by the time the WHO declared a pandemic. In consideration of these facts, we find:
no evidence that the Chinese lockdown had any impact on the trajectory of either Covid cases or deaths.
no evidence that SARS-CoV-2 was highly transmissible.
no evidence that Covid was unusually lethal.
no evidence that anything significant happened in China as a result of Covid (other than the lockdown itself).
nothing that can support the WHO’s decision to consider Covid a pandemic.
Unless the SARS-CoV-2 virus somehow changed its virulence depending on either ethnicity or regional boundaries,[21] we find no reason to think that Covid should have been more lethal in any other country than it was in China. As such, we conclude that there was nothing worthy of being called a pandemic in 2020. Finally, since Covid did not spread out of Wuhan despite five million travellers to other Chinese provinces (a “super-spreader” event of epic proportions), we find no reason to think that it spread out of Wuhan to other countries either.
References
1. Anonymous, “Timeline: WHO’s COVID-19 response,” WHO, 2024, https://www.who.int/emergencies/disease ... -timeline#!
2. Ruiz-Medina BE, Varela-Ramirez A, Kirken RA, Robles-Escajeda E. “The SARS-CoV-2 origin dilemma: Zoonotic transfer or laboratory leak?” Bioessays. 2022 Jan;44(1):e2100189. doi: 10.1002/bies.202100189. Epub 2021 Nov 22. PMID: 34812505; PMCID: PMC8688222.
3. Anonymous, “National Central City,” 2024, https://en.wikipedia.org/wiki/National_central_city
4. Anonymous, “CDC Museum COVID-19 Timeline,” 2024, WHO, https://www.cdc.gov/museum/timeline/cov ... Early-2020
5. He Z, Lv Y, Zheng S, Pu Y, Lin Q, Zhou H, Dong M, Wang J, Fan J, Ye Y, Chen H, Qian R, Jin J, Chen Y, Chen G, He G, Cheng S, Hu J, Xiao J, Ma W, Su X, Liu T. “Association of COVID-19 Lockdown With Gestational Diabetes Mellitus.” Front Endocrinol (Lausanne). 2022 Mar 30;13:824245. doi: 10.3389/fendo.2022.824245. PMID: 35432191; PMCID: PMC9005639.
6. Ren X, Huang W, Pan H, Huang T, Wang X, Ma Y. “Mental Health During the Covid-19 Outbreak in China: a Meta-Analysis.” Psychiatr Q. 2020 Dec;91(4):1033-1045. doi: 10.1007/s11126-020-09796-5. PMID: 32642822; PMCID: PMC7343383.
7. Dong E, Du H, Gardner L. “An interactive web-based dashboard to track COVID-19 in real time. Lancet Inf Dis. 20(5):533-534. doi: 10.1016/S1473-3099(20)30120-1
8. Cheng L, Tan L, Zhang L, Wei S, Liu L, Long L, Zhang J, Wu Y, Zhang Q, Nie S. “Chronic disease mortality in rural and urban residents in Hubei Province, China, 2008-2010.” BMC Public Health. 2013 Aug 2;13:713. doi: 10.1186/1471-2458-13-713. PMID: 23915378; PMCID: PMC3751110.
9. Anonymous, “List of human disease case fatality rates,” 2024, Wikipedia, https://en.wikipedia.org/wiki/List_of_h ... lity_rates
10. Anonymous, “Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19),” 2020, WHO, https://www.who.int/docs/default-source ... report.pdf. Figure 4, p 13.
11. Bristow, Michael, “China’s holiday rush begins early,” 2009, BBC, http://news.bbc.co.uk/2/hi/asia-pacific/7813267.stm
12. Fan J, Hambly BD, Bao S. The Epidemiology of COVID-19 in the Gansu and Jinlin Provinces, China. Front Public Health. 2020 Sep 11;8:555550. doi: 10.3389/fpubh.2020.555550. PMID: 33042952; PMCID: PMC7517784.
13. Leung K, Wu JT, Liu D, Leung GM. “First-wave COVID-19 transmissibility and severity in China outside Hubei after control measures, and second-wave scenario planning: a modelling impact assessment.” Lancet. 2020 Apr 25;395(10233):1382-1393. doi: 10.1016/S0140-6736(20)30746-7. Epub 2020 Apr 8. PMID: 32277878; PMCID: PMC7195331. See Figure 1.
14. Anonymous, “Symptoms of COVID-19,” 2024, CDC, https://www.cdc.gov/coronavirus/2019-nc ... ptoms.html
15. Huang Y, Wu Q, Wang P, Xu Y, Wang L, Zhao Y, Yao D, Xu Y, Lv Q, Xu S. “Measures Undertaken in China to Avoid COVID-19 Infection: Internet-Based, Cross-Sectional Survey Study.” J Med Internet Res. 2020 May 12;22(5):e18718. doi: 10.2196/18718. PMID: 32396516; PMCID: PMC7219722.
16. Molefi M, Tlhakanelo JT, Phologolo T, Hamda SG, Masupe T, Tsima B, Setlhare V, Mashalla Y, Wiebe DJ. “The Impact of China’s Lockdown Policy on the Incidence of COVID-19: An Interrupted Time Series Analysis.” Biomed Res Int. 2021 Oct 28;2021:9498029. doi: 10.1155/2021/9498029. PMID: 34722775; PMCID: PMC8553467.
17. Allen, Douglas W., “Covid Lockdown Cost/Benefits: A Critical Assessment of the Literature,” 2021, SFU, https://www.sfu.ca/~allen/LockdownReport.pdf?
18. Eran Bendavid, Christopher Oh, Jay Bhattacharya, John P. A. Ioannidis, “Assessing mandatory stay-at-home and business closure effects on the spread of COVID-19,” 2021, European Journal of Clinical Investigation, https://onlinelibrary.wiley.com/doi/ful ... /eci.13484
19. Berry CR, Fowler A, Glazer T, Handel-Meyer S, MacMillen A. “Evaluating the effects of shelter-in-place policies during the COVID-19 pandemic.” Proc Natl Acad Sci U S A. 2021 Apr 13;118(15):e2019706118. doi: 10.1073/pnas.2019706118. PMID: 33766888; PMCID: PMC8053946
20. Anonymous, “Crude Death Rate,” 2019, UN-Data, https://data.un.org/
21. Khanijahani A, Iezadi S, Gholipour K, Azami-Aghdash S, Naghibi D. “A systematic review of racial/ethnic and socioeconomic disparities in COVID-19.” Int J Equity Health. 2021 Nov 24;20(1):248. doi: 10.1186/s12939-021-01582-4. PMID: 34819081; PMCID: PMC8611382.
![]() by Belligerent Savant » Thu Feb 29, 2024 10:49 pm
by Belligerent Savant » Thu Feb 29, 2024 10:49 pm
The nature of the events of the Covid era
A detailed summary of PANDA's current understanding
PANDA is committed to open scientific debate and challenging long-held assumptions, and staunchly opposed to the censorship and stifling of critical thinking which characterizes the present day. Our principles assert as much, unequivocally. Science should never be regarded as “settled.” As an organisation we are used to embracing lively debate and new evidence, even to the extent that such inquiry might (and does) falsify core hypotheses we had previously thought were correct.
For instance, in November 2023 we published a revised “vaccine stance” which, though building on work we had done over the past few years, took us to what many regard as a radical position, certainly in comparison to the position we had taken a year before.
It is well known that our material to date is highly critical of governments’ actions over the past 4 years. However, most of our articles, especially those written prior to the past year or so, explicitly or implicitly accept the proposition that there had been an event which justifies the use of the word “pandemic”, and that this had been caused by “the virus”.
In our revised vaccine position, we stated inter alia that in our view the “Covid vaccines” were simply not required because, under any reasonably useful or sensible definition of the word, we had not had a pandemic.
This position statement seeks to set out in more detail what our current thinking is in relation to this relatively new position.
What do we mean by “there was no pandemic”?
The conventional understanding and public perception of a pandemic is one associated with the spread of a disease which a) increases the risk of death for many people, including the previously healthy, and b) directly causes a high number of deaths that would not have otherwise occurred.
Indeed, governing authorities and public health officials implied that everyone, regardless of age and health status, was susceptible to the new virus, anyone could die from it, and that infection by it created substandard immunity which needed augmenting by novel therapeutic injections.
However it quickly became apparent in 2020 that whatever “Covid” was, it did not seem to afflict the healthy any more than many other common respiratory infections, left huge swathes of the planet untouched (even with vast over-attribution), and had no discernible effects on global all-cause mortality.
Hence, under any reasonable and commonly held understanding of the meaning of the word “pandemic”, we were not experiencing one. This is so whether or not a novel virus did emerge at some point prior to 2020 to cause a novel disease referred to as “Covid-19”.
Many of those who insisted we had experienced a pandemic have switched to relying on a meaning of pandemic which does not require that it involves large numbers of deaths, only illness.
However, a wave of largely non-fatal and nondescript respiratory illnesses mainly affecting the elderly and otherwise frail was NOT the basis upon which the establishment justified instituting what turned out to be extraordinarily harmful measures, including the coerced administration of novel therapeutics to billions of people.
Regardless of whether or not what transpired accorded with any entity’s definition of pandemic, it is clear that authorities misled the world – with catastrophic consequences – about the existence of a sudden global health emergency, including the events which preceded and followed the pandemic declaration.
Many have characterised the events of the Covid era as an overreaction to a novel virus which turned out to be less serious than initially claimed, and that serious mistakes were made in the response.
However, we go further than that. We challenge the core assumption underpinning the entirety of most discourse around the subject, as we shall expand upon below.
So, if it wasn’t really a “pandemic”, surely something novel was spreading?
It appears to have become an accepted truth that:
Something novel spread person-to-person from some point directly causing waves of a novel illness.
In 2020 the narrative being promoted was that of a virus with a zoonotic origin which emerged in Wuhan before spreading around the world causing a global pandemic.
More recently, the idea that the zoonotic origin story is false and was being used as a cover-up for the dangerous Gain-of-Function (GoF) research which actually “caused the pandemic” appears to have been gaining traction. It may be significant that, whereas in other respects the mainstream media appears to still be extremely reluctant to report counter-establishment material in relation to the Covid era, the lab-leak theory no longer appears subject to any such censorship.
Our view is that the “lab leak” and “zoonotic spillover” theories are the two constituent parts of a false dichotomy – the presentation of these two options, and the promotion of lively debate solely between them but not outside those parameters, is acting as a distraction from a number of very important questions about the essential nature of the pandemic episode, especially during its early weeks and months.
At present, although there are differences in belief as to where precisely “the virus” originated and how serious an illness it would have caused had authorities “responded better”, there is near-universal acceptance of the following core narrative, including by some of those who have opposed most or all recent government Covid policies:
There was a novel disease caused by a virus which originated from a lab where Gain-of-Function research was being carried out before spreading person-to-person around the world causing a global pandemic.
Not only does PANDA argue against there having been a pandemic, we also do not accept that it has been proven that something novel spread person-to-person from some point directly causing waves of a novel illness.
Is “was there a lab leak” the right question?
Apparently there are hundreds of lab leaks every year. Curiously, none of these have ever seemed capable of causing a significant mass death event, let alone a global pandemic.
So the pertinent question is not “was there a lab leak?” but rather “did a lab leak from a point source result in a virus spreading around the world, suddenly causing lots of people to become sick with a novel illness?”
In PANDA’s assessment, there is no convincing evidence supporting this hypothesis. It is important to note that the establishment narrative requires that all three of these elements be true:
That viruses can be engineered so as to have dangerous pandemic potential.
That the waves of deaths and serious illnesses are linked to the spread of such a virus.
That the virus and disease caused by it are novel, under any rational meaning of that word.
1. Can viruses be engineered so as to have dangerous pandemic potential?
The relationships between sequence, structure and function of viruses are complex and poorly understood. We do not accept that scientists can predict what effect changing a number of base pairs, or inserting some additional genetic material, would have on a virus when it encounters selection pressure in the wild.
We actually doubt that it is possible to create engineered viruses in a laboratory which are, in the real world, replication-competent on a broad scale.
However, even if it were possible to create engineered viruses which are replication-competent, we doubt they could add any significant additional burden of illness or death to the human population let alone do so in such a short timeframe.
Moreover, even if it were possible to create replication-competent engineered viruses which can cause significant illnesses, because of the inverse relationship between contagiousness and virulence whereby all novel viruses rapidly attenuate, such effects are likely to be limited and localised.
We therefore believe that the chance of an engineered virus, which is replication-competent such that it can spread from person to person around the world, causing a dangerous pandemic to the human population globally, is vanishingly small.
2. Were waves of deaths and serious illnesses linked to the spread of such a virus?
The clusters or ripples of illness that would characterise spread of a dangerous contagious pathogen from a point source are not in evidence.
“Pandemic outcomes” differed hugely between neighbouring countries and regions, appearing to obey national, political and administrative boundaries. Differences in the ways in which panic, fear, hysteria spread, and the ways in which harmful pharmaceutical and non-pharmaceutical interventions were applied, are much simpler and more likely explanations for such observations than a spreading pathogen.
With respect to timing, the commencement of the state of “pandemicity” is congruent with the declaration of a pandemic, with no prior signs of abnormality anywhere. Furthermore, there is evidence that the same signal (detected via PCR testing) used to assert viral spread was actually present globally for months before the emergency.
The models developed and used to predict the course of the “pandemic” and inform governments as to what measures they should take are underpinned by multiple baseless assumptions about how viruses spread. In truth, the evidence base regarding mechanisms of transmission for respiratory viral pathogens is extraordinarily thin. This is especially the case for pathogens for which the population has substantial prior immunity.
3. Was there a novel virus causing a novel disease, under any rational meaning of “novel”?
It is simplistic to use this word to refer to “genetically novel” since that would mean every flu was novel. It would also mean that every time there was any mutation of a virus (something which happens with great regularity, even within a single infected person), the result would be a “novel virus”.
The use of the word “novel” by the government officials and agencies which promoted the pandemic narrative conveyed the misleading notion that there was no adequate immune recognition, and that the virus was capable of causing a novel disease with unique characteristics or signatures.
However, whatever SARS-CoV-2 was, there was in fact substantial and effective prior immunity, correlated to the extent of recent exposure to similar coronaviruses. Nearly every healthy person mounted an immune response which was sufficient to prevent serious illness. This is incompatible with any reasonable or useful understanding of the meaning of “novelty”.
We do not accept that there is convincing evidence of a novel disease entity caused by a novel virus. Every characteristic of Covid and all the harms pinned on “the pandemic” can be accounted for by a combination of: the features of known respiratory infectious illnesses; observation and confirmation bias; maltreatment, non-treatment or inappropriate treatment; and other harms consequent to the response to the perception (false, in our view) that a novel deadly virus was circulating.
So what – if anything – did spread?
The starting point in understanding the events of 2020 is acknowledging that whatever the “novel virus” was, it had silently become widespread months before the start of “the pandemic”.
In PANDA’s view, the notion that something then spread during the “pandemic phase” was not driven by person-to-person pathogenic spread but by an extremely rapid ramp-up of PCR testing finding increasing numbers of “positive cases”.
Retrospective analyses of blood (and other) samples collected months before the Covid era consistently found evidence of “the virus” across a wide geographical area. Startlingly, such spread occurred without any reported clusters of unusual illnesses or excess deaths – these only started upon the institution of the response to the assumption that something novel was circulating.
PANDA believes that the rapid rollout of inappropriate, non-specific and oversensitive PCR testing created the illusion that something novel was spreading, whereas in fact all that was truly spreading was the testing itself. In many cases the testing was finding other known or unknown viruses, including those associated with normal seasonal coronavirus waves, whole or fragmented, infectious or not.
As these positive cases were found, a number of perverse incentives created a positive feedback loop, involving more and more testing (especially of “contacts”) being carried out, more “cases” being identified, more testing being demanded, more “cases” being found and so on.
PANDA believes that this conflation of spread of what can be regarded as a mere bystander signal with the spread of a dangerous disease lies at the heart of key conceptual differences between individuals and groups who otherwise share a passion for fundamental human rights and freedom from medical tyranny.
PANDA contends that the harms to health we have witnessed are iatrogenic in nature and/or consequences of the response to the detection of that novel signal, and absent its detection, nothing unusual would have been noticed.
Why does PANDA think this is such an important issue?
PANDA maintains it is a mistake to blame “a virus” when the true culprits are those who fashioned and propagated a false narrative. Using the analogy of John Snow and the 1854 Broad Street cholera outbreak, it is this false narrative – and not a “virus” – which is the pump handle which we need to remove.
As described below, there are dangers inherent in the false narrative currently being enthusiastically embedded in humanity’s psyche. PANDA believes that the best way of insulating us from these is to show that the pandemic was, essentially, a conjuring trick – once the methods of the magicians are revealed, the power of the illusion is lost forever.
Many benefited financially, politically and in other ways from the Covid pandemic narrative, and their ability to continue to do the same for “the next pandemic” does not rely on identifying whether the origin was zoonotic or lab-leak. The perpetrators can continue to argue for the need for a “pandemic preparedness industry” whichever becomes the favoured solution to the “mystery of how the pandemic occurred”.
However, what would be fatal to the future of this lucrative industry is the realisation that we did not have a pandemic at all under any reasonable definition of that word. Hence the extreme reaction to anybody who questions the underlying basis for assuming there was actually a pandemic in contrast to the tolerance shown to those who debate its origin.
The belief that GoF research resulted in a deadly pathogen spreading around the world to create mass illness and death is being used, and will continue to be used, to justify the existence and proliferation of the pandemic and bioterrorism preparedness industries.
Many are demanding that to “prevent the escape of another pandemic-generating GoF virus” we must outlaw GoF research. To be clear, we believe the GoF enterprise is unethical and wasteful, regardless of what it has or hasn’t produced.
History tells us, however, that attempts to enforce moratoria will likely be no more straightforward than previous attempts to outlaw anything once knowledge of it becomes widely distributed. This is especially the case since it is often asserted that any lab can now do this, and the Covid era has, as we have argued above, demonstrated that nothing need actually escape from any lab anyway. The mere seeding of the narrative of escape, rollout of testing and resultant social contagion is all that is needed to perpetuate the perception of a pandemic.
Therefore, if the underlying and false assertion that GoF research can create a global pandemic is not confronted, the spectre of “the next pandemic caused by GoF research” will perpetually hang over humanity like a sword of Damocles.
This will, we predict, result in a relentless march toward more and more draconian measures and pervasive programmes being instituted in the name of “doing better next time”. These will inevitably involve biosecurity surveillance, international treaties to ensure a coordinated global response with stronger and enforceable centralised powers, 100-day vaccine capabilities and the like, all of which are currently being touted as necessary measures.
It is probably not necessary to review the harms and potential harms of such purportedly required measures, other than to remark that their implementation over the past few years was responsible for the transfer of several trillion dollars from the citizenry into the hands of private corporations and other institutions, as well as a variety of other non-financial gains by many actors in the realm of politics, ideology and control.
It is no wonder that those who have profited from all aspects of the Covid narrative would like to retain the rights to this lucrative franchise.
What this statement does NOT say
Firstly, it is not to be read as questioning the existence per se of naturally-occurring viruses. This is not to deny that there are clearly many unknowns with respect to viruses – and the extent of what we don’t know appears to be immeasurably greater than virologists would care to admit. How viruses are transmitted, how and why they infect certain people at certain times and not others, where they come from, how they change, and whether/if they can disappear are poorly, if at all, understood
Secondly, stating that we doubt an engineered virus escaping from a lab caused a deadly pandemic called “Covid” says nothing about any belief around whether bioweapons capabilities exist. Our articles, commentary and this position statement contain no assertions about bioweapons as a general category. Bacterial, bio-chemical, nerve gas and toxicological weapons would seem to be potentially extremely dangerous and all warrant our attention, but not because they can cause pandemics, their effects being localised.
Thirdly, this statement says nothing about what doctors and patients experienced, the nature of illnesses or conditions being treated, or the efficacy of treatments administered. However, in our view the many inconsistencies between these specific observations in specific places, and the story of a novel virus spreading across the world, demand further detailed examination.
![]() by Belligerent Savant » Fri Mar 08, 2024 12:35 am
by Belligerent Savant » Fri Mar 08, 2024 12:35 am
@HansMahncke
·
The CDC "released" a 148 page study on myocarditis after COVID-19 "vaccination" and every single page is completely redacted. This must be a new record.
(b)(5)= Information withheld pursuant to the deliberative process privilege
https://www.documentcloud.org/documents ... oving-foia
https://www.documentcloud.org/documents ... ing-foia-2
![]() by stickdog99 » Tue Mar 12, 2024 4:30 pm
by stickdog99 » Tue Mar 12, 2024 4:30 pm
Users browsing this forum: No registered users and 10 guests
Powered by phpBB® Forum Software © phpBB Group
Site design by Likely Arts based on "Deluxe" by Artodia.