Moderators: Elvis, DrVolin, Jeff
![]() by stickdog99 » Sun Jun 12, 2022 3:48 pm
by stickdog99 » Sun Jun 12, 2022 3:48 pm
![]() by Belligerent Savant » Mon Sep 26, 2022 11:10 am
by Belligerent Savant » Mon Sep 26, 2022 11:10 am
Covid Vaccines Give Prominent "Misinformation"-Fighter's Immune System Cancer
Further examining the case of the anti-anti-vax research leader who got Turbo Cancer after mRNA injection.
Brian Mowrey
18 hrs agoExtremely rare cases like Michel’s create a tricky terrain for science communication. […] In fact, when Michel first told me about his cancer and about the paper he’d written with his brother, I said that I couldn’t write about it. I was worried that some readers would misinterpret my article, and mistakenly see it as a reason not to get vaccinated.
“[Vaccine skeptics are] looking for anything to support their crazy vision,” he said. “It makes me sad about the world in which we are living.”1
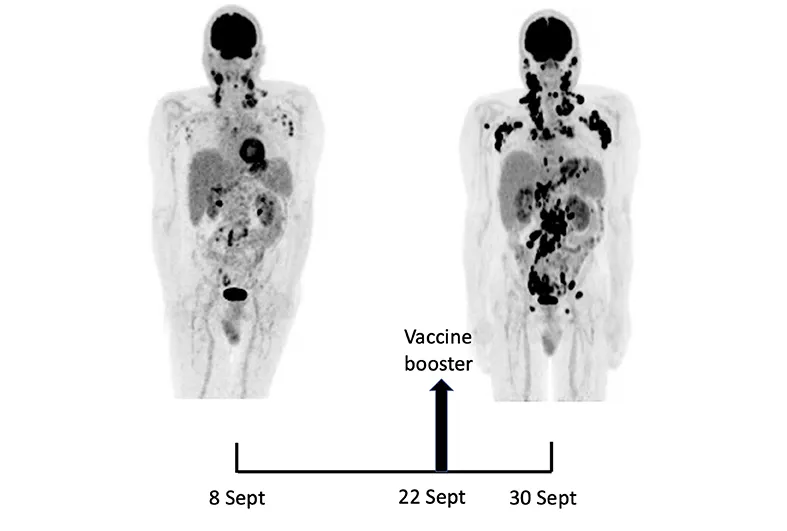
Michel Goldman developed symptoms (first, a flu-like illness, and then night sweats and swollen lymph nodes), and was diagnosed with a rare form of lymphoma in September, 2021. This was 6 months after his initial course of experimental, gene-based injections for SARS-CoV-2 spike protein. The affected, hyperactive lymph nodes were on the same side as the injection arm.
He procured a third injection two weeks after diagnosis, this one into the opposite arm. His symptoms quickly worsened — more intense night sweats, new daytime fatigue, and more lymph node swelling. Eight days later, his lymphoma was found to have expanded with patently unnatural furor, with a particular flourish of activity on the other side of his body than previously affected — the side used for the third injection.
Two months later, in November of 2021, the case report for Goldman, written by himself and his brother, was published at Frontiers in Medicine.2As compared with the initial test, there was a marked 5.3-fold increase in whole-body TLG [a lymph node activity measurement], with the increase in the post-booster test being twice higher in the right axillary region than in the left one.
In February, Jane Ruby used the before- and after-third dose comparison from this paper to advocate against taking the experimental, gene-based injections for SARS-CoV-2 spike protein.
This makes Goldman “sad about the world in which we are living.”
As opposed to, you know, seemingly getting cancer because of his Covid vaccines.
“We Can’t Handle the Truth”
Goldman’s story was reluctantly reported in The Atlantic yesterday by Roxanne Khamsi, who initially “said that I couldn’t write about it.”
Khamsi is a career science journalist™ who has written hundreds of articles, served as chief editor for Nature Magazine for over 10 years, and has taught science journalism™ at Stony Brook University and CUNY.3
So, is not being able to write about vaccine adverse events a full class, or just a chapter? How many times has Khamsi “couldn’t” write about adverse events, or “couldn’t” publish them as editor?
And yet this astonishing admission of journalistic malpractice is just tossed-off, as easily and naturally as Sam Harris endorsing full-blown state censorship if the thing being censored is a populist former President.I was worried that some readers would misinterpret my article, and mistakenly see it as a reason not to get vaccinated.
Why shouldn’t I refuse to write about Goldman’s adverse reaction, reads the subtext to Khamsi’s admission: After all, isn’t preventing anti-vaxxers from thinking vaccines are unsafe more important than evaluating whether vaccines are safe?
The irony lost on Khamsi is that a career science journalist™ being consciously reluctant to honestly broker the case for the risks of vaccines is itself a valid reason to believe vaccines are unsafe.
I do not say this in the context of concern-trolling over “trust” or “reputation;” this is a question of rampant, religious delusion: If the “pro-vaccine” side has to censor adverse events to “win” the case, it is a signal that they have succumbed to dogma.
It is not the only such signal in this sad story.
Goldman, for example, leads “I3H,” an organization devoted to the Nonsense Speak mission of “Fostering Interdisciplinarity.”4 I3H takes a meta-approach to promoting new ways to drug up all of humanity, dipping its toes in regulatory streamlining, promotion of neglected treatment strategies (including monoclonal antibodies for infection with SARS-CoV-2), pro-vaccine and -lockdown indoctrination of children,5 and gathering intelligence that coincidentally fosters the future dismantling of vaccine-skeptical information networks.
And so when Goldman, “innovative healthcare”-promotor, comes down with lymphoma out of the blue 6 months after his first two injections with an “innovative healthcare,” it doesn’t even occur to him that this itself is an adverse event.
After all, most adverse events happen within a few days of injection; we know this because when they happen after 6 months we don’t even consider them as possibly related, because after all most adverse events…
Goldman’s Type of Cancer is Associated with Recent Immune System Provocation
https://unglossed.substack.com/i/748993 ... rovocation
Goldman’s new cancer was Angioimmunoblastic T-Cell Lymphoma — affected lymph nodes crowd up with hyperactive Follicular Helper T Cells, along with some characteristic accumulations of Follicular Dendritic and EBV-gene expressing B Cells which may be mere bystanders.
It typically occurs after age 60 (Goldman was 66).Most people develop AITL in their 60s and 70s. 6
While it may be primed by somatic mutations to T Cells, it is believed to typically be provoked by some sort of recent immune insult.The exact, underlying cause of AITL is unknown. It is believed that a dysfunctional immune system response to an unknown antigen ultimately leads to the development of the disorder. 7
As opposed to the carcinogenic dangers that might apply to the populace as a whole,8 manifestation or progression of AITL after Covid-vaccination suggests that Follicular Helper T Cells were primed to "go crazy" upon the mere presentation of mRNA-encoded spike protein within lymph nodes. In fact, this is exactly the mechanism Goldman and co-authors propose for the observed explosion in activity after the third dose:In fact, the supposed enhancing action of the vaccine on AITL neoplastic cells is fully consistent with previous observations identifying TFH cells within germinal centers as key targets of nucleoside-modified mRNA vaccines [but only after the third dose?]
Hilariously, they comment on the “interesting” fact of a previous paper not considering the link:Regarding the relationship with the underlying malignancy, hypermetabolic lymph nodes were considered as malignant in 5% of the patients while no conclusion regarding the malignant nature could be drawn in 15% of the vaccinees including 16 patients with lymphoma. Interestingly, in none of these studies [nor by us, here, regarding my first two doses], the possibility that the mRNA vaccines could have played a role in the development of malignant lymph nodes was considered.
And so Goldman, — who doesn’t report being infected with SARS-CoV-2 until the next February — must either ascribe his lymphoma to some other immune insult, or to his injection with mRNA for the spike protein. It is ridiculous to simply rule out the latter. There is not in fact a biological law that prevents adverse events from manifesting months after the fact; this is a secular religious fantasy.
Wouldn’t it make sense that what can exacerbate in the third dose, could have instigated in the first two?
Neither in his original paper nor his dialogue with Khamsi is the question even brought up. Perhaps Khamsi can post a follow-up with additional “anti-vax” online statements lamentably inspired by her Actually Doing Journalism For Once. If so, please include:Goldman, you clearly got cancer from the Covid vaccine to begin with.
Notwithstanding this staggering blind-spot, Goldman advocates for more robust attention to “rare” adverse events. As Khamsi reports, there was much hesitation and hand-wringing on his part. Although eventually pulling the trigger and publishing his case-report, he is picky with his language, and refuses to consider his experience to imply any risk to anybody outside of incredibly exotic birds of pre-disposition such as himself.Whatever the result of [prospective studies screening for adverse events only in rare AITL patients], it should not affect the overall favorable benefit-risk ratio of these much-needed vaccines.
Well, of course not — because that would require acknowledging that prospective screening of all sorts should have taken place in everyone to begin with, during the trials.
Khamsi presents Goldman as a tortured mind who, when faced with an imagined moral dilemma — will searching for the truth empower those who question vaccines? — sided with the truth. Again, the admission that both Goldman and Khamsi, powerful brokers of scientific knowledge, are instinctually reluctant to acknowledge adverse events, and this means they may have suppressed other reports, isn’t even apparently realized.
Why should it be suspicious that a lifelong vaccine promoter and lifelong scientific interlocutor waited until he, himself, was the victim?
Neunez, M. Goldman, M. Goldman, S. Lambert, PH. (2019.)
Confessions of a Vaccine Idolater
Khamsi’s essay is not done divulging insights on the dogmatic, dissonance-strewn mindset of vaccine idolaters.
In the dialogue between her and Goldman:When we talked about the potential side effects of the AstraZeneca vaccine last year, Michel made it clear that, in the big picture, any chance of serious complications from the shots would be orders of magnitude smaller than the chance of complications from the pandemic illness itself.
Based on what?If COVID vaccines caused clotting disorders or myocarditis in a tiny percentage of those who received them, he assured me, COVID would lead to stroke or heart inflammation in a much larger group.
Based on what?Or maybe the cancer and the mRNA vaccine were connected, but the risk of getting immunized was still just a tiny speck beside the benefits.
Based on what?
In every case, the mere property of being called a “vaccine” seemingly activates an axiomatic feature of the universe that magically prevents negatives from outweighing benefits.
And just what do our fanatics imagine the “benefits” actually are, in this case?He remains adamant that COVID-19 vaccines are necessary and useful for the vast majority of people.
If the “vast majority” of people do not suffer severe infection or death from encounter with SARS-CoV-2, what necessity or use is there in injecting them with mRNA for spike protein in advance? But in this religion, of course, the axiomatic demands exerted on the universe by the magic word “vaccine” ensure that “at least one, anywhere” constitutes a “vast majority.”
The fact is that a majority of people survive infection without severe outcomes, even in “high-risk” groups. They fight off the infection with their immune system and they move on. Injections that reduce severe outcomes do not benefit people who wouldn’t have experienced them to begin with; they are therefor of no use to most people. And even if a plurality of people suffer long-term symptoms after infection — what evidence is there that injection improves this rate? It is mixed, at best;9 the reality might be that these injections cause the same symptoms just as often.10
Khamsi closes with reflection. Goldman’s lymphoma apparently responded to treatment (leaving aside the question of whether it might have self-resolved). He has made his call for expanded pharmacovigilance which in no way should be taken as questioning the mighty glory of the god Vaccine.
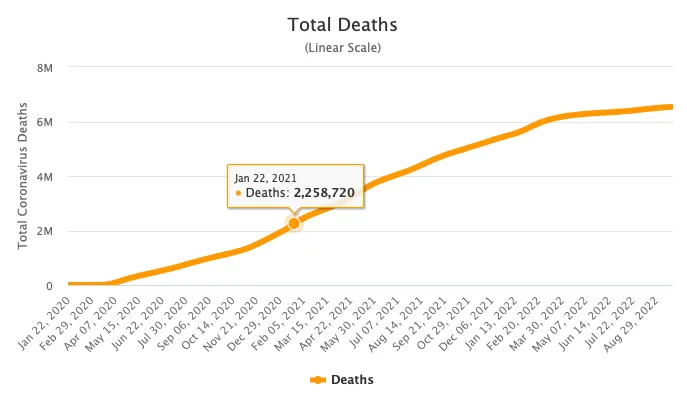
And yet, naturally, he wrests with the question of what it means that the god Vaccine did, in fact, smite him. The only solution to this problem, it seems, is to believe in the god’s wonders for humanity at large even more fervently.[Goldman is now questioning whether] a vaccine that is saving tens of millions of lives each year might have put his own in jeopardy.
This is a frankly unhinged number, suggesting a psychotic break with reality on the part of our vaccine idolators.
https://www.worldometers.info/coronavirus/worldwide-graphs/
Worldwide deaths including obvious denial of therapeutics and case-inflation.
As well as an unsupportable use of present participle in the Omicron era. But even granting a fantasy of complete death protection resulting from worldwide, universal uptake — steelmanning the case for these failed injections as much as possible — how can Goldman and Khamsi actually be sure that injecting 8 billion, yearly or bi-yearly, to save 3 million, is actually a net positive? A rate of 4 deaths in 10,000 from yearly injection would lead to a net negative.
How does Goldman know that isn’t the rate? As he recently irresponsibly opined in his case study:It is therefore unlikely that existing pharmacovigilance systems will be efficient to identify extremely rare cases
Thanks to the axiom-enforcing magic of the word “vaccine,” of course, the math doesn’t actually matter. “Vaccine” will self-correct reality: Ah, look, the experimental injections are saving 100 million now, and every hour at that!
Goldman may have lapsed into self-martyrdom rather than renouncing his god, but in clinging to the god in the first place he is clearly projecting himself onto the public at large. If he thinks he needed this awesome toxic, experimental, poorly-monitored, cancer-inducing, cancer-promoting protection against SARS-CoV-2, then everyone — the vast majority — must need it, too. Can’t have a “vast” majority without children. Lets get this ridiculously untested product into them, too. Parasitic elderly germaphobe vampires gonna parasitic elderly germaphobe vampire.While Michel remains unsure about his fourth shot, he has continued to be outspoken on the benefits of vaccination overall, and often speaks to Belgian media on the topic.
Take it already, you reckless, misinformation-spewing menace to Vaccine!
----------------------------------------
1
Khamsi, Roxanne. “Did a Famous Doctor’s COVID Shot Make His Cancer Worse?” (2022, September 24.) The Atlantic.
(Emphasis added.)
2
Goldman, S. et al. “Rapid Progression of Angioimmunoblastic T Cell Lymphoma Following BNT162b2 mRNA Vaccine Booster Shot: A Case Report.” Front Med (Lausanne). 2021 Nov 25;8:798095.
3
https://ca.linkedin.com/in/roxanne-khamsi
4
http://i3health.eu/wp-content/uploads/2 ... ion_HD.pdf
5
Neunez, M. Goldman, M. Goldman, S. Lambert, PH. (2019.) “Vaccines, Shots That Protect You.” Front Young Minds. 7:31.
Stevens, H. Neunez, M. (2020.) “COVID-19, The Quarantine-Virus Disease.” Front Young Minds. 8:102.
These do have a bit of entertainment value in so far as representing attempts to be “hip” with the “kids” by throwing entire walls of text at them (complete with “abstracts”).
6
https://rarediseases.org/rare-diseases/ ... -lymphoma/
7
ibid.
8
See “Liquid Cancer.”
9
See “The Protective Effect” (database-based evidence for ‘Long Covid efficacy’) and “The BA.5 Summer Survey Study” (survey-based evidence for ‘Long Covid inefficacy’).
10
Patterson, et al. “SARS-CoV-2 S1 Protein Persistence in SARS-CoV-2 Negative Post-Vaccination Individuals with Long COVID/ PASC-Like Symptoms.” researchsquare.com
jaovista
16 hr ago
·
Am I allowed to go on a limb here and think , just for second, that the Atlantic journalist might be in reality a whistleblower trying to come across as a propagandist, a Trojan horse of sorts in mainstream media? Would that be too farfetched?
You rightfully and wittingly demolished the article -content and characters- the contradictions, lack of logic and blatant propaganda. Still for me it seems that anyone reading that article, or just skipping over - the last thing they would do would be to get another booster, that article wrote cancer and vaccine in the same sentence. This association is what the Atlantic reader would be left with regardless of the article "packaging"
FYI: There is another substack dealing with the Atlantic article (got there before yours from one of Igor's DEBATE comments https://wholistic.substack.com/p/mrna-c ... mainstream)
And I liked better the original title. Thank you for your work.
Brian Mowrey
16 hr ago
An intriguing theory!
I am inclined to bet that Khamsi, after her initial impulse to squash the story, decided or was goaded by editors into presenting it as a [Red Scare voice] "Pity us reasonable science-believers! We WANT to discuss (super-duper rare!) adverse events, but those icky ANTI-VAXXERS won't LET us!" story. This is consistent with the current RTs on her twitter feed: Nothing else to do with her weekend but RT people congratulating her for her nuanced take, apparently. But the audience (engagement with the tweets she is RT'ing) doesn't seem eager to appreciate her work.
Thank you for a vote for the original title, haha.
jaovista
16 hr ago
·
Nonetheless I'd rather see people having (kinda late) epiphanies than these-so-rare-side-effects.
...
Modern Discontent
17 hr ago
The Goldman scenario always seemed rather interesting. It's been a while since I looked at the first case report and I don't remember much about his history but it does raise questions as to why that didn't, in some regard, provide for a perfect opportunity to examine him and see what could be going on.
There's a serious issue in which reporters may obfuscate facts or information for fear that the public may not react properly. It just reminds me of my August post and the idea that the public plays a serious role in what science gets presented and what science gets funded. But it's also a reminder that researchers and scientists can be rather hubris and act in a manner that they deem acceptable due to their position and authority.
Out of all of the cancer possibilities lymphoma seems to be one that's worth heavily investigating, although I would like to see more of Goldman's prior medical history to have some frame of reference.
Igor Chudov
16 hr ago
The "journalists" are afraid of their grave responsibility for participating in a campaign to poison millions. They are not blind to that fact
Barney Rubble
17 hr ago
·
There are many signals that cancers are exploding. The amount of folks within our degrees of separation that have recently been diagnosed with cancer, and even died suddenly, is anecdotally stunning.
And obviously hence the reason they had to bastardize the definition of vaccine.
Realistic
17 hr ago
Thank you. You are totally correct. Some pathologists tried to sound the cancer and vaccine alarm last year but they keep getting silenced. Even when I was an undergrad in virology class, the esteemed prof said every vaccine has side effects and some will not be know for years. Suddenly Fauci and friends dismiss all side effects except a sore arm. But the public has discovered the trick, just look at the pitiful mouse booster numbers.
Jon
17 hr ago
The circularity of their logic is breathtaking.
It's too dangerous to consider that the downsides of the vaccine might outweigh the upsides, because that might lead to fewer people taking it. That would be a disaster, because we KNOW the upsides outweigh the downsides, because otherwise it wouldn't have been right to make so many people take it. So we don't need to even consider it, which would anyway be dangerous because...
There needs to be an M.C. Escher style staircase showing their logic path.

![]() by Belligerent Savant » Mon Sep 26, 2022 12:37 pm
by Belligerent Savant » Mon Sep 26, 2022 12:37 pm
Review Article
Curing the pandemic of misinformation on COVID-19 mRNA vaccines through real evidence-based medicine - Part 1
Aseem Malhotra
Journal of Insulin Resistance | Vol 5, No 1 | a71 | DOI: https://doi.org/10.4102/jir.v5i1.71 | © 2022 Aseem Malhotra | This work is licensed under CC Attribution 4.0
Submitted: 10 June 2022 | Published: 26 September 2022
About the author(s)
Aseem Malhotra, Public Health Collaboration, London, United Kingdom
Abstract
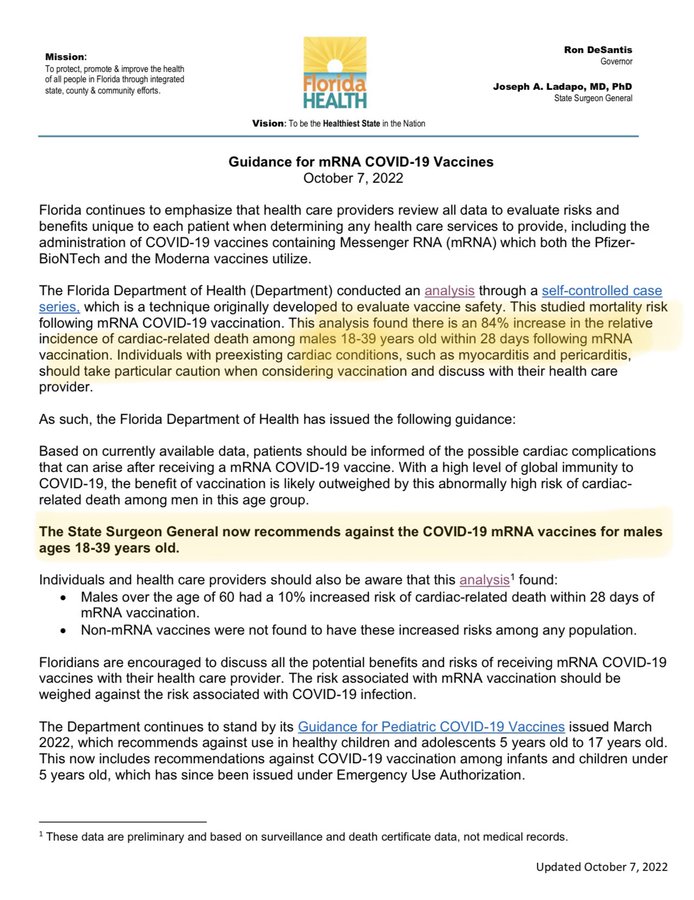
Background: In response to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), several new pharmaceutical agents have been administered to billions of people worldwide, including the young and healthy at little risk from the virus. Considerable leeway has been afforded in terms of the pre-clinical and clinical testing of these agents, despite an entirely novel mechanism of action and concerning biodistribution characteristics.
Aim: To gain a better understanding of the true benefits and potential harms of the messenger ribonucleic acid (mRNA) coronavirus disease (COVID) vaccines.
Methods: A narrative review of the evidence from randomised trials and real world data of the COVID mRNA products with special emphasis on BionTech/Pfizer vaccine.
Results: In the non-elderly population the “number needed to treat” to prevent a single death runs into the thousands. Re-analysis of randomised controlled trials using the messenger ribonucleic acid (mRNA) technology suggests a greater risk of serious adverse events from the vaccines than being hospitalised from COVID-19. Pharmacovigilance systems and real-world safety data, coupled with plausible mechanisms of harm, are deeply concerning, especially in relation to cardiovascular safety. Mirroring a potential signal from the Pfizer Phase 3 trial, a significant rise in cardiac arrest calls to ambulances in England was seen in 2021, with similar data emerging from Israel in the 16–39-year-old age group.
Conclusion: It cannot be said that the consent to receive these agents was fully informed, as is required ethically and legally. A pause and reappraisal of global vaccination policies for COVID-19 is long overdue.
Contribution: This article highlights the importance of addressing metabolic health to reduce chronic disease and that insulin resistance is also a major risk factor for poor outcomes from COVID-19.
Keywords
COVID-19; mRNA vaccine; cardiac arrests; real evidence-based medicine; shared decision-making
![]() by guruilla » Thu Oct 13, 2022 3:50 am
by guruilla » Thu Oct 13, 2022 3:50 am
The COMUSAV Mexico (World Health and Life Coalition, subsidiary Mexico) is an organization that brings together more than 3,000 doctors from 14 countries who practice a protoloc based on CDS Chlorine Dioxide to successfully treat Covid-19.
COMUSAV Mexico is headed by Dr. Pedro Chávez Zavala, President, and Dr. Manuel Aparicio, Vice President. The organization has made public studies that demonstrate how to treat Covid-19 with Chlorine Dioxide CDS. The mineral is also a highly efficient treatment for other diseases.
________________________
-----------------------------------------
COMUSAV Mundial (Spanish acronym for World Health & Life Coalition) is the largest organization supporting the therapeutic use of Chlorine Dioxide Solution worldwide. Working w/the Scientific Community to legalize it in every country! https://t.me/s/OfficialChannelComusavUSA
Presentation in 2 days: https://eventos.comusav.com/
Home website: https://comusav.com/en/
![]() by guruilla » Thu Oct 13, 2022 5:02 am
by guruilla » Thu Oct 13, 2022 5:02 am
This Artists United for Life promo has got that C0$ feel to it.
https://www.comusav.com/en/concierto/
It's meant to look bigger/more popular than it actually is. Tweets are stale.
https://twitter.com/ComusavMundial
https://twitter.com/comusav
Almost nothing on youtube:
https://www.youtube.com/channel/UCbg1d9 ... Z-Eit0f_UA
https://www.youtube.com/watch?v=CxxI3lceBOI
Up to date on Telegram tho -62.5K subscribers:
https://t.me/s/comusav
Found a number of dead links like this one to Mik Anderson's blog: https://corona2inspect.net/2022/05/08/r ... icaciones/
Archived here - sourced nanotech research at some of these links:
ttps://web.archive.org/web/202205151219 ... icaciones/
https://web.archive.org/web/20211217131 ... x_tr_hl=es
https://web.archive.org/web/20220102204 ... gspot.com/
https://web.archive.org/web/20211018204 ... gspot.com/
It looks serious actually and several "captures" by internet archive have "been removed":
https://web.archive.org/web/20220119071 ... log&bpli=1
graphenevaccine
graphenevaccine
20211202_Blogger_censors_C0r0n_@_2Inspect's_article_about_nanorouter.pdf
Mik Andersen, author of http://www.corona2inspect.blogspot.com
´Dear friends and subscribers of C0r0n @ 2Inspect. This morning Blogger has censored your blog of reference, canceling the publication of the following articles: 1) Pattern identification of patterns in c0r0n @ v | rus vaccines: nanorouters # 2) Identification of patterns in c0r0n @ v | rus vaccines: nanooctopuses and carbon-graphene nanotubes # 3) Identification of patterns in blood of vaccinated people: GQD graphene quantum dots.
I have published a short entry with a reflection on the matter. I want to thank you for your support and help. What has happened here is proof that in this Blog we have come close to the truth, that they are even capable of censoring scientific work. They don't want people to question, think, or analyze the situation. They have an interest in settling any scientific debate, any report, any information that goes against their plans. C0r0n @ 2Inspect has fulfilled its mission successfully, since it has managed to transfer the evidences and tests that demonstrate the great lie of our times. Thank you all once again.´
t.me/graphenevaccine/2189
Here is the documentation for the tech in the film: https://www.comusav.com/wp-content/uplo ... dersen.pdf
La Quinta Columna has been following and reporting: https://rumble.com/LaQuintaColumna
But they are also pimping a story about super "black-eyed babies"?: https://www.bitchute.com/video/gjkzHY40LNua/
Too much!
![]() by Grizzly » Fri Oct 14, 2022 1:16 am
by Grizzly » Fri Oct 14, 2022 1:16 am

![]() by Belligerent Savant » Sun Feb 19, 2023 9:31 pm
by Belligerent Savant » Sun Feb 19, 2023 9:31 pm
Dangerous mRNA Vaccine Contaminants Were Just Discovered
A Discussion on Production Quality Control, Bacterial Evolution, Spike Proteins and Antibiotics
A Midwestern Doctor
3 hr ago
The current mission of this Substack has been to prove fraud on the vaccine manufacturer’s part. This is because I believe it is the most persuasive point for sinking the entire COVID-19 vaccine program as it gives those who blindly supported the narrative a way to save face if they pivot (“it’s not my fault, Pfizer lied to me”) and because proven fraud is the most likely thing to make governments act against the manufacturers.
If you consider the situation with Operation Warp Speed (using an untested technology to design a vaccine for an extraordinarily difficult pathogen to make a vaccine against in a fraction of the time it takes to make a normal vaccine), it should be obvious there was no reasonable way to accomplish its goals. Instead, the best that could be done would be to cut a lot of corners and hope whatever incomplete vaccine came out could be pushed onto the market without too many issues subsequently emerging.
Since you aren’t supposed to cut corners during the pharmaceutical development process, the only option was to conceal all of this that happened (also known as fraud). Interestingly, when I completed my review of what was seen by each whistleblower at Pfizer, I learned the company has a long and documented history of sweeping things under the rug and deleting or altering incriminating documents.
With the COVID-19 vaccines, the likely points of fraud were:
•Producing preclinical data (e.g., animal studies) that claimed the vaccines were safe and effective.
•Altering the clinical trials to erroneously claim the vaccines were safe.
•Altering the clinical trials to erroneously claim the vaccines were effective.
•Producing the claimed vaccine product (there were quite a few almost insurmountable production challenges for doing this).
In a recent article, I reviewed how this issue was systemic throughout the clinical trials (e.g., those severely injured by the vaccine were aggressively gaslighted by the study coordinators so their adverse events could be dismissed from the final results). Similarly, I also recently reviewed some of the other signs Pfizer submitted fraudulent data to regulators on the production quality of their final vaccine product.
Since the time that article was written, more signs have also appeared confirming that Pfizer (and likely the other manufacturers) are not accurately reporting what is in their vaccine. One of the most recent discoveries is particularly compelling because it helps to explain some of the observations quite a few of us have seen in vaccinated patients.
Spike Protein Persistence
Many of us who have worked with vaccine-injured patients suspect that the COVID-19 vaccine can persist for an extremely long time in their bodies (which makes it quite challenging to treat them). One of the best points of evidence for this theory is autopsy studies of suspected vaccine deaths where spike proteins are found throughout the tissues months after their vaccination.
However, exactly why this happens is a bit more of a mystery, and as far as we know the half-life of the mRNA vaccines was never tested prior to them entering the market. Before the recent citizen’s investigation, I had the following potential explanations for what was happening:
•Because the mRNA was modified to resist degradation in the body (so it could produce sufficient vaccine product) and the manner used to do this (pseudouridation) is quite haphazard, it is very likely some of the vaccine mRNA persists for months inside the body. The only study that has ever looked at this issue found it was still present 60 days after vaccination and did not look further into the future.
•The mRNA is changing the DNA of cells and causing them to begin permanently produce spike proteins. Research has now shown that mRNA alters the DNA of cells, but it is not clear if this change is enough to cause significant and sustained spike protein production throughout the body.
•Some vaccinated individuals (e.g., those who develop myocarditis) cannot form antibodies to the spike protein, and this causes the vaccine spike proteins to persist for a very long time within the body.
•The vaccine eliminates the body’s ability to eliminate a COVID-19 infection, and as a result, a chronic low-grade COVID-19 infection develops which continually manufactures spike proteins in the body.
mRNA Vaccine Quality Control
One of the major challenges with producing the mRNA vaccines was how many complex steps with a propensity for error needed to be done correctly to create the finalized product. A few of these were:
•Producing the correct DNA plasmids (those that would result in spike protein mRNA being made).
•Giving them to E. coli bacteria which then begin reproducing those plasmids, which are then harvested and transformed into DNA that can be used to make the spike protein-producing mRNA.
•Eliminating everything except the intended mRNA from that mixture so that it could be packaged into the lipid nanoparticles for the final vaccine product.
Although there have been many signs that the final mRNA product was not what Pfizer and Moderna advertised, to my knowledge no one has directly tested the genetic sequences present. Fortunately, the technology to do so is widely available, and recently an anonymous Substack did just that. One of its most interesting discoveries was that the DNA plasmids were still present at a much higher concentration than the arbitrary threshold set by drug regulators (Pfizer was the worst offender). This has a lot of very important implications we will discuss after a brief interlude.
Antibiotics
Antibiotics are one of the modern-day miracles of medicine and their ability to save lives has fundamentally improved our modern lifestyle to a degree most have difficulty even comprehending in the current era. Conversely, since antibiotics were first discovered, practitioners from many different medical systems have noticed that they seem to cause a variety of issues that can outweigh the benefits of the therapy. Most of these issues are encapsulated under the belief that antibiotic therapy trades an acute disease for a chronic one. In general, the issues tend to fall under one of the following:
•Antibiotics are toxic to mitochondria (mitochondria evolved from bacteria and share many similarities to them).
•Individuals can have allergic reactions (although this is the most obvious issue, it typically has the most minimal long-term consequences for a patient).
•Antibiotics have a high degree of general toxicity which typically results in them being pulled from the market once safer options are made available (sadly this can often take years).
•Antibiotics pathologically disrupt the microbiome and bacterial evolution.
Unfortunately, in conventional medical practice, most of these issues are not recognized, and the focus instead always goes to determining which drug the bacteria are least likely to have antibiotic resistance towards (as this is what medical training primes you to focus on). This bias frequently results in dangerous and not necessarily needed antibiotics being prescribed as “allergies” and antibiotic availability are typically the only contraindictions considered. In short, there are a lot of issues that arise from antibiotics being given out like candy.
Although I try to minimize my usage of pharmaceuticals, and there are a variety of effective non-pharmaceutical therapies for infections, antibiotics are nonetheless sometimes needed. From having looked at the above question in detail, I believe the safest antibiotics you can somewhat reliably address things they are needed for are as follows:
•Ceftriaxone (Rochephin)
•Doxycycline
•Azithromycin (the Z-Pack)
•Cefalexin (Keflex)
For those curious, the first antibiotic is a first-line therapy for many infections patients require hospital care for (so I always keep some in my closet), the first three treat many complex conditions caused by chronic infections (e.g., Lyme disease or Garth Nicolson’s mycoplasmas), and the last two treat many common infectious illnesses.
Additionally, there are a few other antibiotics (Ciprofloxacin is the best example) that are dangerous but sometimes are nonetheless needed to treat life-threatening infections. Unfortunately, those drugs (Ciprofloxacin again being the best example) are also given out for much more minor infections you can treat with other antibiotics (e.g., a urinary tract infection) due to the medical community being unwilling to acknowledge their dangers.
Medical Models
For the institution of science to progress, it needs to have a standardized way to teach the discipline to future members. In turn, one of the major challenges with science is the immense complexity of nature as the complexity present will often exceed whatever can be taught within a standardized model. When you add in the human ego, this often leads to “science,” becoming anti-science (opposed to the scientific process of inquiry) because those who invested themselves in the standardized paradigm taught to them are frequently unwilling to consider a more complex universe that calls the simplistic paradigm they were taught into question.
Due to the immense complexity of the human body mind and spirit, this issue is particularly apparent within medicine. To address this complexity, every medical system has taken a similar approach: create a simplified model of the human body which allows one to identify key areas that can be focused upon to create a positive effect for the patient.
The perspective of healthcare practitioners radically changes once they begin to employ multiple models rather than simply the one they were trained in. Assuming one is open-minded, they normally realize:
•Certain models come much closer than others to encompassing the wide range of medical needs of each human being.
•That for each medical issue there are normally multiple models which have a viable means to address it.
•For each of those issues, there is typically one model that is dramatically better than the others (e.g., there are a few conditions that I believe should always be treated with Traditional Chinese Medicine).
The above also is true within the medical system. Specialists from the same medical specialty will default to treating many patients they see nearly identically, but when a patient sees specialists from another specialty, they will often be given a completely different regimented treatment approach. For example, this is commonly observed by patients with a chronic debilitating illness like Lyme disease or chronic fatigue syndrome when they see cookie-cutter rheumatologists and neurologists.
Similarly, within the integrative field, you will commonly observe integrative physicians become very committed to a specific approach or holistic model and treat everyone within their box. Each of these boxes works for some (but by no means all patients).
It is thus very difficult to find physicians who use a wide range of boxes and are willing to creatively discern which box fits best for their patient’s needs. Similarly, colleagues who run integrative clinics have told me one of the greatest challenges they face is finding physicians they can hire who will go outside their specific box and do not need formulaic protocols to follow. Because of all of this, it is extremely common to see patients with a complex illness see dozens of providers before they are lucky enough to stumble upon one whose box fits their medical needs.
Bacterial Homeostasis
A very common box integrative medicine practitioners utilize is focusing on the gut microbiome, since “good” bacteria produce a variety of essential biomolecules, while “bad” bacteria produce a variety of toxins that can dysregulate the entire body. Books could be written on all the approaches available for addressing the gut microbiome, but most of them essentially boil down to lab tests to determine if your microbiome is abnormal, agents to eliminate bad bacteria, probiotics, and prebiotics, and dietary changes to support a healthy gut microbiome. It should also be noted there are many other important microbiomes in the body besides that within the gut that can also become dysregulated and create significant issues when they do (e.g., on the skin, in the urinary tract, in the vagina, in the eyes, on the skin, etc.).
One of the general beliefs within this discipline is that “bad” bacteria tend to have a much greater antibiotic resistance than “good” bacteria, so when you utilize an antibiotic for something like an ear infection, it also kills off the good bacteria that previously kept the bad bacteria in balance, allowing the bad ones proliferate and take over the gut flora. While this is true, I believe there is also an entirely separate mechanism that explains why this pathologic transformation occurs.
Note: The next two parts of this article will likely be highly controversial—please look past them if you feel this way.
When you attempt to observe what goes on inside the blood or in tissues with microscopes, two major issues always arise for observing bacterial organisms.
•Light physics makes it nearly impossible for an optical microscope to resolve (clearly distinguish) specimens smaller than 150-200 nanometers, and while this is sufficient to see most common bacteria, many microorganisms are much smaller than this (e.g., mycoplasma, the smallest bacteria, are 1–2 μm long and 0.1–0.2 μm wide, while SARS-CoV-2 is a sphere 0.07 μm to 0.09 μm in diameter). The alternative, electron microscopy requires everything observed to be fixed and killed, so it is not possible for living processes to occur under the electron microscope and many of these smaller components often become distorted by the fixation process.
•There is an immense degree of variability in the forms of bacteria of the same species, many of which can appear to the untrained eye to be something else (e.g., irrelevant cellular debris).
One of the major (but mostly forgotten debates within medicine) regards the morphology (shape) of bacteria. One of the schools (the conventional one) believes they maintain a relatively constant morphology (except for times when they do things like forming spores). A different school believes that their morphology can significantly vary, and this variation is often heavily influenced by the surrounding environment of the body (this is where terrain theory comes from).
I believe the still unresolved disagreement between these two schools of thought (which has persisted for over 150 years) exists for three reasons:
•The technological limitations of optical microscopy (as many of the pleomorphic bacterial forms are too small to see with conventional microscopy).
•Pleomorphism existing adds an overwhelming degree of complexity to understanding microbiology. It is hence much easier to come up with reasons to dismiss signs of the pleomorphic nature of bacteria (and certain other microorganisms like fungi) than it is to seriously study them.
•The monomorphic paradigm is much more amenable to pharmaceutical management (and in many cases, it works).
Advocates of Pleomorphism
There are a few well-known figures who advanced this model. Two, Gaston Naessens and Royal Rife (both now deceased) developed optical microscopes with clever designs that could bypass the optical magnification limit. Under those microscopes, they observed a complex biological cycle of pleomorphic organisms (e.g., this one) which appeared to be influenced by the surrounding terrain.
Although these ideas are quite controversial, I am inclined to support them. This is because both scientists demonstrated immense integrity throughout their lifetimes and both utilized their microscopic observations to develop remarkable (but mostly forgotten) therapies I have repeatedly observe work in clinical practice. Simultaneously, however, I do not believe the cycles they mapped out were completely accurate, as they resemble but do not match what later researchers using modern techniques found, which is completely understandable given that Naessens and Rife were simply researchers working alone on an immensely complex topic.
The most recent well-known advocate of pleomorphism was Lida Mattman, who in 2006 published, Cell Wall Deficient Forms: Stealth Pathogens. It is a compilation of dedicated researchers using modern microbiology techniques (e.g., antibody staining, chemical analysis, a variety of culturing techniques, careful electron microscopy, etc.) whose data demonstrates the pleomorphic nature of bacteria and the behaviors of those forms. It should be noted these researchers also identified pleomorphic fungi, and that bacteria could sometimes adopt a fungal-like morphology (which some bacteria are also conventionally recognized as doing), but for length considerations, those fungi will not be discussed further here.
One of the best theories I have seen to explain all of the contradictory observations about cancer is that the cancer process is an ancient survival response of cells. In this model, when stressed by an environment the cell cannot survive in, some of the cells rather than dying, revert to a more primitive evolutionary stage. One of the things that characterize increasing evolutionary development is cells becoming able to work in harmony with each other for the sake of a greater whole, and conversely when the opposite occurs the cells focus on their own benefit at the expense of the surrounding organism. As a result, once cells become cancerous, if allowed to, they will grow out of control and destroy the surrounding organism with which they should be in harmony.
A similar thing appears to occur with bacteria (and some fungi—e.g. candida has been observed changing its morphology depending on what carbohydrates are available to it). When these organisms are stressed by environmental factors, while many of the organisms die, many others are incompletely killed and instead revert to a more primitive form.
Frequently for example, the bacteria lose their cell walls and become mycoplasma-like cell wall deficient organisms (CWD or L-form bacteria) with similar but not identical characteristics to the original organism. A variety of stressors can trigger this transformation, but antibiotics that target the cell wall of a bacteria (e.g., penicillin) are the most effective for inducing this transformation.
Once the transformation occurs, the CWD bacteria become much harder to detect (most conventional microbiology techniques cannot culture them, and like viruses, they pass through most bacterial filters). Eventually, once a sufficient number of them are present (which requires a safer environment without the previous stressor), they will revert to their classical form.
As a result, numerous infections that follow a chronic relapsing pattern or that are difficult to determine if one is or is not infected with them can be observed to have CWD bacteria present when the infection is in “remission” and not conventionally detectable (e.g., with skip cultures). Similarly, when CWD bacteria are still detected, this can often accurately predict the occurrence of a relapse. It should also be noted that both CWD and classical bacteria are typically both present and frequently inhibit the growth of the other (presumably to ensure the appropriate balance of each).
CWD organisms often end up residing within cells (as they are better suited to surviving that environment). Because they reside within cells, they often provoke an autoimmune response to the cells they reside within (which is essentially a less severe version of what is now being seen in autopsies of vaccine victims where the immune system attacks cells containing spike proteins). In a variety of different autoimmune diseases that have no known “cause,” such as scleroderma, sarcoidosis, lupus, a variety of kidney diseases, uveitis, “non-infectious” ulcers, arthritis, ulcerative colitis, Crohn’s disease, and multiple sclerosis, cell wall deficient bacteria have been identified by researchers, often directly within the cells of the affected tissues. In some cases, a very specific CWD organism is tied to the condition, while in others, multiple ones are found.
CWD bacteria are also found in certain autoimmune conditions after the infection is assumed to have passed (e.g., group a strep is known to cause rheumatic fever, and CWD strep can be found in the affected heart valves of someone with rheumatic fever). CWD bacteria have also been found in certain cancers, blood clots, kidney stones, and atherosclerotic plaques. In some of the diseases listed, it is only the CWD form that creates disease (e.g., in rats Streptococcus fecalis was innocuous when injected into rabbit ileum, whereas the CWD variant caused granulomas).
This is an immensely interesting subject, and I would highly recommend anyone who wants to learn more to read Mattman’s book (it contains all of the references for the above section and much, much, much more such as the pleomorphic nature of the bacteria which causes Lyme disease). I also felt one of Mattman's statements excellently summed up the entire phenomena:While many points remain obscure, cell wall deficiency and variation are clarified when one views classical growth as perfect cooperation between wall autolysis and replacement. Aberrant forms result whenever there is imperfect balance between construction and destruction.
One of the most well-known scientists who advanced the pleomorphic model was Günther Enderlein, who due to the era he lived in did not yet have access to advanced microscopic technologies and instead had to make do with a lot of observation, intuitive explorations, and careful deliberation. In 1925, he published a summary of his work outlining a pleomorphic cycle of organisms he observed traces of within the blood. Enderlein essentially argued that when these organisms were in a healthy environment, they had a symbiotic relationship with the body, whereas when they were in an unhealthy environment, they created disease.
The existence of microorganisms in the blood is a hotly debated subject since blood is conventionally considered to be sterile (whereas I believe hard-to-detect CWD bacteria are often present). One of the better cases I’ve seen against the sterility of the blood was contained within one of the classic books every ICU doctor learns from:The organisms involved in CRBI [Catheter-related bloodstream infection] are (in order of prevalence) coagulase-negative staphylococci, Gram-negative aerobic bacilli (Pseudomonas aeruginosa, Klebsiella pneumoniae, E. coli, etc), enterococci, Staphylococcus aureus and Candida species (40). Coagulase-negative staphylococci (mostly Staphylococcus epidermidis) are responsible for about one-third of infections, while Gram-negative bacilli and other organisms that inhabit the bowel (enterococci and Candida species) are involved in about half the infections. This microbial spectrum is important to consider when selecting empiric antimicrobial therapy.
This quote demonstrates that microbes from the bowel can colonize the catheter, and therefore must be present to some degree in the blood.
Enderlein came up with a very creative approach to addressing pathologic regulations of the pleomorphic cycle which completely diverges from the Allopathic mindset. First, he would try to fix the terrain of the body. Secondly, he would culture the pleomorphic organisms when they were in a healthy state, create a dilute extract of them (which became the Sanum isopathic remedies), and then expose organisms in an unhealthy state to that extract, at which point they would transform to the healthy state.
Enderlein’s approach appeared to work, so it has maintained a devoted group of adherents for almost a century which combines healing of the terrain with the Sanum remedies. I personally believe that the full program is not practical for most patients, but some of the isopathic remedies by themselves (when correctly administered) are remarkably effective for treating certain otherwise difficult-to-treat conditions (although in many cases they are not alone sufficient to treat the condition). Some of those conditions include:
•Systemic Lupus Erythematosus
•Gut and urinary microbiome dysregulation following the administration of certain antibiotics such as fluoroquinolones or Flagyl.
•Mastitis and prostatitis.
•Many types of cancers.
As I discussed in the previous series on zeta potential, I believe that one of the primary causes of blood clumping and poor zeta potential is pleomorphic dysregulation, and in some cases, you cannot address the coagulation issue unless the underlying microbial issue is also addressed. Many of the above authors have likewise made this observation (e.g., Naessens found the non-pathologic form of his pleomorphic cycle was distinctively negatively charged, Mattman’s work details pleomorphic organisms found within thrombi and that when one bacteria became CWD, it could cause kidney stones, the formation of which is heavily influenced by zeta potential).
Similarly, one of the remedies Enderlein developed targeted a pleomorphic organism he believed was responsible for blood clotting, and in practice, this one often helps conditions characterized by poor circulation and increased blood viscosity. One of the interesting things we have discovered from working with COVID-19 and vaccine injuries is that this isopathic remedy is also often very helpful for improving the circulatory issues observed following a spike protein injury. This and other observations have led us to believe one of the issues with the spike protein vaccines is them disrupting the homeostatic regulation of the pleomorphic microbiome.
Note: One of the frequent misunderstandings I see from advocates of terrain theory who attack germ theory and the existence of viruses on Substack, is failing to recognize the two theories are not mutually exclusive. A dysregulation in one’s terrain can cause illness, and the introduction of a pathogenic microbe can also cause illness.
Spike Proteins and the Microbiome
Viruses (besides bacteriophages) do not typically infect bacteria. One of the many odd characteristics of COVID-19 however is that it does (I first learned about it from this post which discussed an Italian study that demonstrated how it happens). This is important since a sustained infection of the gut microbiome with SARS-CoV-2 can transmit the virus into your stools and sustain its presence within the body.
The researcher who has studied this phenomenon the most is Dr. Sabine Hazan M.D. a gastroenterologist and researcher who has built her career around researching the gut microbiome. Throughout the pandemic, Hazan has observed that unhealthy changes in the gut microbiome predisposed one to a severe COVID-19 infection and that SARS-CoV-2 infects the gut microbiome (many of her studies are published here).
More importantly, Hazan has also observed that COVID-19 vaccination pathologically alters the gut microbiome so that the bacteria she had found would typically prevent a severe COVID-19 infection (and many other conditions) disappear. As far as I know however, she has not put forward a definitive explanation of why this happens (the best guess I have heard from Hazan was that the spike protein produced by the vaccines is a toxin that kills the good bacteria).
One of the things that are not appreciated about bacteria is how incredibly well-suited they are to adaptation and developing the complex enzymes that make life possible. Bacteria rapidly reproduce in large numbers, allowing them to have an almost infinite number of opportunities to make the needed evolution, and then once one does, it shares that DNA with the surrounding bacteria (via plasmids), making it possible for a bacteria colony to rapidly adapt to its environment. This likewise is why it is often so hard to deal with bacteria simply by targeting them with lethal agents.
When I examined Enderlein’s isopathic remedies (the ones extracted from healthy microorganisms and then given to unhealthy ones to positively transform them), I concluded that their active ingredient was most likely plasmids. Thus, when these plasmids were taken up by the pathogenic organisms, they would both transform the pathogenic ones to a healthy state and then cause the bacteria to reproduce and have the healthy plasmid before long be produced throughout the body.
Like Hazan, until I saw the recent citizen’s investigation, it had not occurred to me that we might just be directly transfecting the gut microbiome with a spike protein plasmid (and essentially giving the equivalent of a toxic isopathic remedy).
Other Plasmid Modifications
In addition to the spike protein, it was also noted that the plasmids found contained the gene for the SV40 virus promoter (I am still unsure of the implications of this) and resistance to kanamycin and neomycin (interestingly, these are some of the antibiotics CWD bacteria are the most susceptible to). Inserting this resistance in addition to the target modification is done as a method of ensuring that bacteria that ultimately reproduce contain the desired genetic modification (as the other bacteria are purged by those antibiotics). This approach however is strongy advised against since it creates the potential for antibiotic resistance (a major issue in infectious disease control) as those genes can eventually make it to populations of bacteria outside the laboratory (along with many other issues).
Conversely, however, an additional issue emerges here; if an individual who has spike protein-producing bacteria within their microbiome is exposed to these (and potentially similar antibiotics) it will rapidly select for them to only have those bacteria. There are in turn some reports on VAERS of adverse reactions in vaccinated individuals following the administration of these antibiotics.
If you have the time, I would highly recommend reviewing this investigation and Jessica Rose’s follow up to it, both of which have a much greater focus on the technicalities of what was found within the vaccines and additional points of evidence supporting fraud by the vaccine manufacturers.
Conclusion
One of my great disappointments is the many Democrats who vocally spoke out against all the potential safety issues with vaccines produced within the timeline Operation Warp Speed was operating under who completely changed their tune once Biden was elected and they decided to push it on America.
It is still difficult for me to believe that we were all told to “trust the experts” on the vaccine, but we were never permitted to directly evaluate its data or evaluate what was actually in the vaccines, especially since there were a variety of extremely valid concerns regarding what could potentially be in them. Instead, we just were left hanging and left to deal with the inevitable problems that emerged.
Note: East Palestine, Ohio is essentially dealing with an identical situation now to this with the train derailment that had large amounts of toxic chemicals be “safely” burned in their vicinity while the residents have been left to wait and see what complications they will develop.
Since the start of the rollout, many people were seriously concerned about the potential quality control issues with the vaccines, and from almost the start of the vaccine rollout, it has been abundantly clear there are serious issues which are leading to a high variability over what ends up in each vaccine. Typically within the pharmaceutical industry, this is absolutely inexcusable. However, as you all know the exact opposite has happened and people aren’t even allowed to independently examine the products.
Since there are so many things that could have gone awry, despite a lot of research on the subject, I genuinely admit I had not even considered this possibility there could be plasmid contamination adversely transforming our entire microbiome. However, as I hope this article has shown, in hindsight, it makes a great deal of sense. All of this should illustrate just how many serious issues can happen when an experimental vaccine is rushed to market and critical steps (such as sufficiently removing the bacterial plasmid from the final product) are skipped—especially with a gene therapy.
As you might guess, these quality control issues were particularly apparent with my favorite pharmaceutical company:While the Moderna vaccines are meeting this specification [the maximum allowable plasmid contaminant level originally proposed by regulators], the Pfizer [vaccines] are 10-fold higher in contamination with 1 DNA molecule per 350 mRNAs. This is 1 replication competent plasmid per 350 mRNA molecules and equates to billions of antibiotic resistant plasmids injected per person per shot.
![]() by Grizzly » Wed Feb 22, 2023 8:41 pm
by Grizzly » Wed Feb 22, 2023 8:41 pm
Holy smokes!
In a peer review science journal Fauci co-authored a report talking about the "incomplete and short-lived" protection provided by the mRNA vaccines.
The biggest rat of them all is fleeing the sinking ship.
![]() by Belligerent Savant » Thu May 11, 2023 4:31 pm
by Belligerent Savant » Thu May 11, 2023 4:31 pm
Kevin McKernan
@Kevin_McKernan
·
May 9
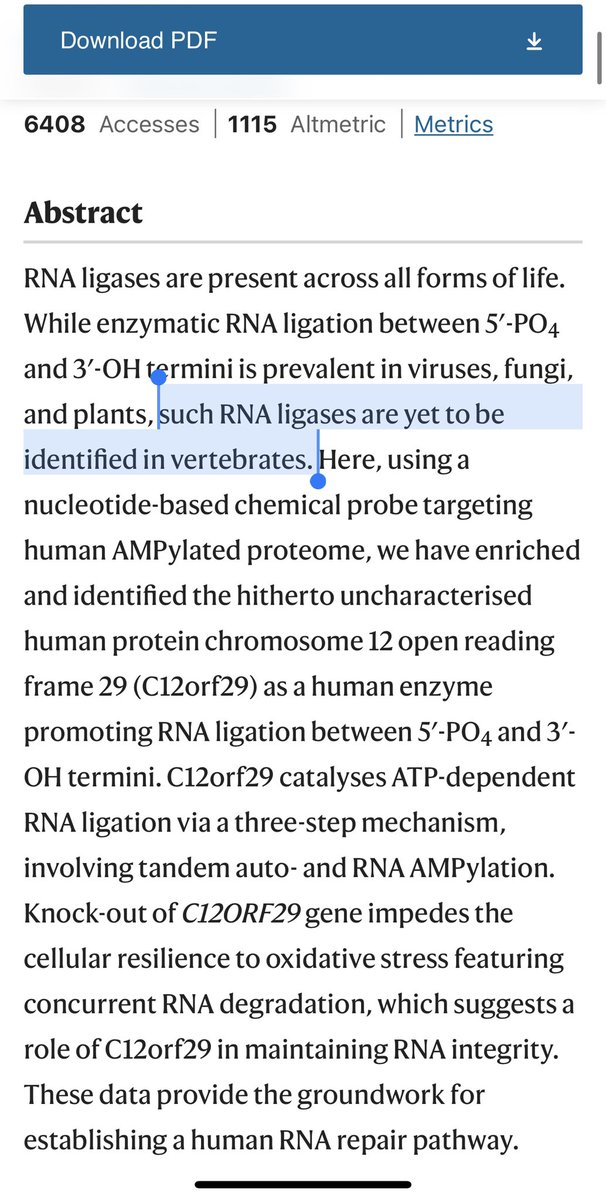
After billions of people have been injected with novel mRNAs,
We’re just learning about a human RNA ligase we didn’t know about.
https://www.nature.com/articles/s41467-023-36451-x
Chemoproteomic discovery of a human RNA ligase
Yizhi Yuan, Florian M. Stumpf, …Andreas Marx Show authors
Nature Communications volume 14, Article number: 842 (2023)
This wasn’t an expected unknown.
They have not found ligases like this in Vertebrates.
This is a major discovery.
…
@Eriker91947663
How is the vaccine different from the virus?
…
Differences in Vaccine and SARS-CoV-2 Replication Derived mRNA: Implications for Cell Biology and Future Disease
Kevin McKernan1*, Anthony M. Kyriakopoulos2and Peter A. McCullough3,1Medicinal Genomics, Beverly Mass, USA; Kevin.McKernan@medicinalgenomics.com 2Nasco A.D. Biotechnology Laboratory, 11 Sacthouri Str. 18536 Piraeus, Greece;rnd@nascoad.com 3. Truth for Health Foundation, Tucson, AZ, USA;peteramccullough@gmail.com*Correspondence: kevin.mckernan@medicinalgenomics.com
Abstract:
Codon optimization describes the process used to increase proteinproduction by use of alternative but synonymous codon changes. In SARS-CoV-2mRNA vaccines codon optimizations can result in differential secondaryconformations that inevitably affect a protein’s function with significantconsequences to the cell. Importantly, when codon optimization increases the GCcontent of synthetic mRNAs, there can be an inevitable enrichment of G-quartetswhich potentially form G-quadruplex structures. The emerging G-quadruplexes arefavorable binding sites of RNA binding proteins like helicases that inevitably affectepigenetic reprogramming of the cell by altering transcription, translation andreplication. In this study, we performed a RNAfold analysis to investigate alterationsin secondary structures of mRNAs in SARS-CoV-2 vaccines due to codonoptimization. We show a significant increase in the GC content of mRNAs in vaccinesas compared to native SARS-CoV-2 RNA sequences encoding the spike protein. Asthe GC enrichment leads to more G-quadruplex structure formations, these maycontribute to potential pathological processes initiated by SARS-CoV-2 genetic vaccination.
https://osf.io/bcsa6/
RNA ligases participate in repair, splicing, and editing pathways that either reseal broken RNAs or alter their primary structure. Bacteriophage T4 RNA ligase (gp63) is the best-studied member of this class of enzymes, which includes yeast tRNA ligase and trypanosome RNA-editing ligases.
![]() by Belligerent Savant » Mon May 29, 2023 5:09 pm
by Belligerent Savant » Mon May 29, 2023 5:09 pm
Dr. Eli David
@DrEliDavid
·
Breaking: New peer-reviewed paper published in the journal Vaccines finds that repeated Covid boosters:
- May INCREASE risk of severe Covid illness (instead of reducing it)
- May increase risk of cancer growth and autoimmune disease
IgG4 Antibodies Induced by Repeated Vaccination May Generate Immune Tolerance to the SARS-CoV-2 Spike Protein
by Vladimir N. Uversky 1,*ORCID,Elrashdy M. Redwan 2,3ORCID,William Makis 4 andAlberto Rubio-Casillas 5,6ORCID
Abstract
Less than a year after the global emergence of the coronavirus SARS-CoV-2, a novel vaccine platform based on mRNA technology was introduced to the market. Globally, around 13.38 billion COVID-19 vaccine doses of diverse platforms have been administered. To date, 72.3% of the total population has been injected at least once with a COVID-19 vaccine. As the immunity provided by these vaccines rapidly wanes, their ability to prevent hospitalization and severe disease in individuals with comorbidities has recently been questioned, and increasing evidence has shown that, as with many other vaccines, they do not produce sterilizing immunity, allowing people to suffer frequent re-infections. Additionally, recent investigations have found abnormally high levels of IgG4 in people who were administered two or more injections of the mRNA vaccines. HIV, Malaria, and Pertussis vaccines have also been reported to induce higher-than-normal IgG4 synthesis. Overall, there are three critical factors determining the class switch to IgG4 antibodies: excessive antigen concentration, repeated vaccination, and the type of vaccine used. It has been suggested that an increase in IgG4 levels could have a protecting role by preventing immune over-activation, similar to that occurring during successful allergen-specific immunotherapy by inhibiting IgE-induced effects. However, emerging evidence suggests that the reported increase in IgG4 levels detected after repeated vaccination with the mRNA vaccines may not be a protective mechanism; rather, it constitutes an immune tolerance mechanism to the spike protein that could promote unopposed SARS-CoV2 infection and replication by suppressing natural antiviral responses. Increased IgG4 synthesis due to repeated mRNA vaccination with high antigen concentrations may also cause autoimmune diseases, and promote cancer growth and autoimmune myocarditis in susceptible individuals.
![]() by Pele'sDaughter » Tue May 30, 2023 7:12 am
by Pele'sDaughter » Tue May 30, 2023 7:12 am

![]() by Belligerent Savant » Tue May 30, 2023 9:28 am
by Belligerent Savant » Tue May 30, 2023 9:28 am
New Onset Multiple Sclerosis Post-COVID-19 Vaccination and Correlation With Possible Predictors in a Case-Control Study
Majed Alluqmani
Published: March 18, 2023
DOI: 10.7759/cureus.36323
Peer-Reviewed
Abstract
Introduction: Various inflammatory diseases have been associated with the administration of various vaccines. Several reports have associated vaccine administration with the demyelinating diseases of the central nervous system (CNS). However, no clear or strong scientific evidence exists to support the association of vaccine administration with the onset of demyelinating diseases. Some CNS demyelination diseases such as acute disseminated encephalomyelitis (ADEM) and neuromyelitis optica spectrum disorders (NMOSD) were reported following the administration of COVID-19 vaccines. In this study, new onset multiple sclerosis (MS) following COVID-19 vaccine administration was reported.
Methods: In this longitudinal observational case-control study, a total of 65 participants were studied, who were divided into two groups. Group A included 32 MS patients who were diagnosed post-COVID-19 vaccine administration and group B included 33 participants who received COVID-19 vaccines and did not develop MS. Group B was used as a control. The Chi-square test and logistic regression analysis were carried out using Statistical Product and Service Solutions (SPSS) (IBM SPSS Statistics for Windows, Armonk, NY) software.
Results: Univariate and multivariate logistic regression analysis was performed and a significant correlation between the risk factors and the development of MS post-COVID-19 vaccination was identified.
Conclusion: The risk factors, identified in this study, can be used as significant independent predictors for developing MS post-COVID-19 vaccinations.
![]() by stickdog99 » Tue May 30, 2023 1:46 pm
by stickdog99 » Tue May 30, 2023 1:46 pm
![]() by Pele'sDaughter » Wed May 31, 2023 8:01 am
by Pele'sDaughter » Wed May 31, 2023 8:01 am
Users browsing this forum: No registered users and 5 guests
Powered by phpBB® Forum Software © phpBB Group
Site design by Likely Arts based on "Deluxe" by Artodia.