8. Evidence of corruption or undue influence in our health institutionsMedical journals and researchers
Is it a problem that doctors, scientists, medical journals, teaching hospitals, and university medical schools can accept money from the pharmaceutical industry?
A former editor of the British Medical Journal describes how Pharma can cleverly use medical journals to its own advantage. And this review article investigates whether Pharma funding leads to more outcomes favorable for the funder (spoiler alert: it does).
Is it a problem that when drug companies submit their trial data to science journals, they own the data, and the peer reviewers and editors of the journal don’t get to actually see the raw data? So they have to take the drug companies for their word?
And is it a problem that most doctors don’t seem to know this?
Again, from the interview with Dr. John Abramson:
When a drug company sponsors a clinical trial, and they do the analysis and they write up a manuscript… and they send it to a medical journal and it gets peer-reviewed, and doctors are trained that they should trust peer-reviewed articles and that’s how the system works. The peer-reviewers and the editors of the medical journals don’t get to see the data. They have to take the word of the drug companies that they’ve presented the data accurately and reasonably completely. And you only get to see it in litigation, five years later…
He goes into more detail on this in his book Overdosed America, which I highly recommend.
By the way pharmaceutical companies also give money to the editors of prestigious medical journals. And many medical journals depend on the drug industry to pay for advertisements. Advertising is an important revenue stream for these journals, and industry spent a combined $637 million in 2016 to buy ads in medical journals, the majority of which were ads to market drugs to doctors.
More on the influence that Pharma has on medical journals and academic investigators here, here, here and here.
And watch an interview on this topic with Dr. Marcia Angell, Harvard Medical School faculty member and former editor-in-chief of the New England Journal of Medicine: here.
Global health organizations
There are various global health organizations like the WHO, as well as non-profits and “public-private partnerships” that have enormous influence over global health. A discussion of them could fill a multivolume book, but I’ll just list some useful links here:
Corruption in global health: the open secret
Covid-19, trust, and Wellcome: how charity’s pharma investments overlap with its research efforts
Private research funders court controversy with billions in secretive investments
WHO: Do financial contributions from ‘pharma’ violate WHO Guidelines?
L’OMS: Bateau ivre de la santé publique (translation: The WHO: Drunken boat of public health)
WHO Voluntary contributions by fund and by contributor, 2020
Who is really helping the WHO?U.S. health institutions
The pharmaceutical/health products industries spent $266 million on lobbying in Washington in 2021 alone.
A 2007 study in the Emory Corporate Governance and Accountability Review summarized how compromised federal health officials have transformed the NIAID, NIH, CDC, and FDA into Pharma subsidiaries.
And here’s a 2019 report on the corporate capture of our policymakers.
Let’s dig into specific institutions.
The FDAThe FDA is responsible for protecting the public health by assuring the safety and efficacy of drugs and other products.
They do not test drug themselves. Drug manufacturers get to test their own drugs, and submit their results to the FDA to review. More here.
The FDA used to be entirely funded by taxpayer money, but today nearly half of the FDA’s budget comes from the very companies it is supposed to regulate.
FDA advisers can accept money from pharmaceutical companies, which creates incentives to “play nice” with them.
Drug companies can buy access to invitation-only meetings where they can meet with FDA officials and possibly influence them.
Roughly 32% of drugs approved by the FDA between 2001-2010 were later found to have a safety issue, according to a Yale-led study. The FDA has had a history of approving unsafe drugs, and all signs point to the problem getting worse.
The FDA (and other institutions) can make journalists compliant.
The FDA has promised “full transparency” on Covid vaccines. And yet, a group of more than 30 scientists and doctors had to sue the FDA to get it to release all the data and documents it relied upon to license Pfizer’s Covid vaccine.
The FDA’s response? First, it asked a federal judge for 55 years to fully release the data. That’s a rate of 55 pages per month. Then later, the FDA doubled down and asked for 75 years to fully release the data.
This, despite the fact that it took precisely 108 days for the FDA to review all the documents throughly enough to ensure that the Pfizer vaccine was safe and effective for licensure.
Luckily, the federal judge recently rejected the FDA’s request and ordered them to produce all the data at a rate of 55,000 pages per month. We’ll see what’s in those documents, but the first batch of documents released reveals that Pfizer actually had to hire more people in order to keep up with tracking all the adverse events being reported.
We already mentioned Maddie de Garay earlier, in the “2- Testimonies from the vaccine injured” section. As mentioned, her life-altering injuries were ignored by the FDA (as well as the CDC and NIH):
FDA Buries Data on Seriously Injured Child in Pfizer’s Covid-19 Clinical Trial
The FDA should not authorize the Pfizer jab for younger children until it conducts a proper trial
Aaron Siri
Oct 22, 2021
Speaking of kids, when the FDA was deciding on whether to approve Pfizer for children, a voting member of the FDA advisory committee admitted that we wouldn’t know how safe the Pfizer Covid vaccine was until we started administering it. His exact words were: "We're never gonna learn about how safe the vaccine is unless we start giving it. That's just the way it goes." Video here.
Two top FDA officials, including the head of the FDA’s vaccine center, resigned back in Septermber, and it was speculated that it was over the issue of political pressure to authorize boosters in young people. In fact, the FDA chose to bypass its expert advisory committee and authorize boosters for children between 12 and 15 years of age.
At least the FDA is consistent: recently the FDA and CDC advised boosters for Omicron when (1) there is no clinical data supporting it, (2) in the past they had said they would not accept vaccine efficacy less than 50% and (3) Omicron, by all accounts, appears to be much milder than the previous strains and it’s unclear whether we need a vaccine for it. More here:
Vinay Prasad, MD MPH
@VPrasadMDMPH
Pre Vax 2020, FDA said they would not accept vaccine efficacy less than 50% (minimum bar)
Ontario data now suggesting a 3rd dose (booster) has Vax effectiveness of 37% for Omicron
Yet FDA & CDC advising booster FOR omicron?
A Few thoughts..
There’s a “revolving door” between Pharma and regulatory agencies. If regulators can leave the FDA for high-paying Pharma jobs, they might go easy on pharmaceutical companies in order to stay in their good graces.
I wonder if this is an example:
HEALTH AND SCIENCE
Former FDA Commissioner Scott Gottlieb joins Pfizer’s board of directors
https://www.cnbc.com/2019/06/27/former- ... board.htmlRecently, Biden picked Dr. Robert Califf as FDA Chief, despite the fact that he’s made millions as a consultant in the pharmaceutical industry and holds millions more in Pharma investments (see here or here).
We could go on, but hopefully you get the point.
The CDCThe CDC is supposed to “protect America from health, safety and security threats, both foreign and in the U.S.”
Remember the V-Safe app data I mentioned earlier in the “3- Evidence from medical records or official databases of adverse events” section?
The CDC is being sued to release that data to the public. Apparently it contains 119 million entries.
Like the FDA, the CDC receives money from companies. This is often under the guise of “public-private partnerships.”
Here’s a list of their partners.
The list not only includes pharmaceutical companies like Pfizer, Johnson & Johnson, Merck, and Gilead, but also includes Facebook, Google, McDonalds and Coca-Cola.
Just like with other regulatory agencies, there’s a revolving door. Example here.
The CDC’s Advisory Committee on Immunization Practices (ACIP), which sets the U.S. adult and childhood immunization schedules, is full of members that own vaccine patents or stock in vaccine companies, or receive money from vaccine manufacturers.
More here, for an overview of some of the conflicts of interests, and even accounts of data manipulation.
The Office of Inspector General, which is responsible for reducing fraud or abuse of our regulatory agencies, found that the CDC often didn’t comply with its own ethics requirements (see here and here).
A Congressional Government Reform Committee report criticized the FDA and CDC for routinely allowing scientists with conflicts of interest to serve on the advisory committees that influence vaccine policy.
In 2016, The Hill published a letter by more than a dozen senior CDC scientists charging that the agency was participating in research fraud.
In 2010, there was a scandal where Congress found that the CDC had deliberately manipulated scientific documents about the safety of Washington D.C. drinking water.
The CDC seems to have a cozy relationship with Pfizer.
I mentioned earlier that the CDC has said that they would be investigating the death of 13-year old boy Jacob Clynick; see page 2 of these emails, which were obtained by Judicial Watch. That was over 6 months ago.
More examples of kids whose deaths are being ignored here.
Like the FDA, the CDC is also pushing for boosters, despite no supporting clinical data. In fact, they don’t seem data-driven at all. As Dr. Marty Makary put it:
Remarkably, despite having 21,000 employees, the CDC is still unable to provide the key COVID statistics we need to inform public policy. The agency has not released data on natural-immunity reinfections, and chief Rochelle Walensky falsely said on “Fox News Sunday” that with Omicron, “prior infection protects you less well” than vaccination. I’d love to see that data.
Most alarming, two years into the pandemic, the CDC has not been able to tell us how many people are in the hospital for COVID versus with COVID. Reports from New York City and Miami Jackson Memorial Hospital are among many finding that the majority of COVID hospitalizations are primarily for other conditions — but when patients are admitted and tested, they’re found to have an incidental COVID infection.
More on how Covid deaths are counted and manipulated: here.
Speaking of a lack of data, why do we still not know what proportion of the U.S. population has already been infected with SARS-CoV-2? It wouldn’t be that difficult to randomly sample people for evidence of past infection. Wouldn’t this be useful information to know?
Reminder that the CDC budget is over $8 billion.
Then there’s evidence of sheer ineptitude. Here was an account from biologist Joanna Masel, on how frustrating it was to deal with CDC staff:
@JoannaMasel
Many are torn between frustration and sympathy for
@CDCgov
. Given all the things CDC are failing to get done (eg rapid data dissemination and analysis), I am shocked by what they DO they spend time on. sharing observations from my interactions with CDC staff. 1/14
More here:
@alexandrosM
Break up the CDC.
Data gathering and transparent reporting should be firewalled from advocacy.
They have a treasure trove of data, and they use it to p-hack propaganda. Anything useful we learn is from Israel, UK, and Scandinavia.
And disease is sure not getting controlled.
By the way, the CDC director recently hired a PR firm. They’re gonna need it.
The NIH & NIAIDThe National Institute of Allergy and Infectious Diseases (NIAID) is part of the National Institutes of Health (NIH). The NIAID is supposed to conduct and support “basic and applied research to better understand, treat, and ultimately prevent infectious, immunologic, and allergic diseases.”
Since Dr. Anthony Fauci took charge of the NIAID in 1984, the prevalence of chronic allergic and autoimmune disease has only increased.
Instead of researching the causes of this explosion of allergic conditions, Fauci has funneled most of his $6.1 billion budget to the development of new drugs. He promotes the relationship with Pharma as a “public-private partnership” (see 34:06 here).
Pharmaceutical companies routinely pay extravagant royalties to Dr. Fauci and his employees at NIAID.
See:
Biomedical Research:NIH Should Publicly Report More Information about the Licensing of Its Intellectual Property
Report: Researchers mumon financial interests
Royalty payments to staff researchers cause new NIH troubles
Information for NIH Inventors
The way it works is as follows: first, NIAID begins the process of drug discovery in its own labs. Then clinical trials for these drugs are farmed out to a network of some 1300 academic “principal investigators” (PIs), or researchers, who conduct the human trials at university-affiliated research centers and hospitals. These PIs receive funds from the NIAID. Then after these researchers develop a potential new drug, NIAID transfers some or all of its share of the intellectual property to private pharmaceutical companies, through HHS’s Office of Technology Transfer. The researchers (PIs) and their universities can also claim their share of the patents, which cements their loyalty to the NIAID (and Fauci).
Once the drug gets to market, the pharmaceutical company pays royalties through an informal scheme that allows Pharma to funnel profits from the drug sales to the NIAID officials who worked on the product. This is essentially a form of legalized kickbacks.
So Dr. Fauci and his employees personally pocket money from drugs they helped developed at taxpayers’ expense.
Emails that were obtained via a Freedom of Information Act request made by the group American Institute for Economic Research (AIER) revealed that Fauci and the NIH director Francis Collins colluded to shut down dissenting views on lockdowns from highly credentialed epidemiologists.
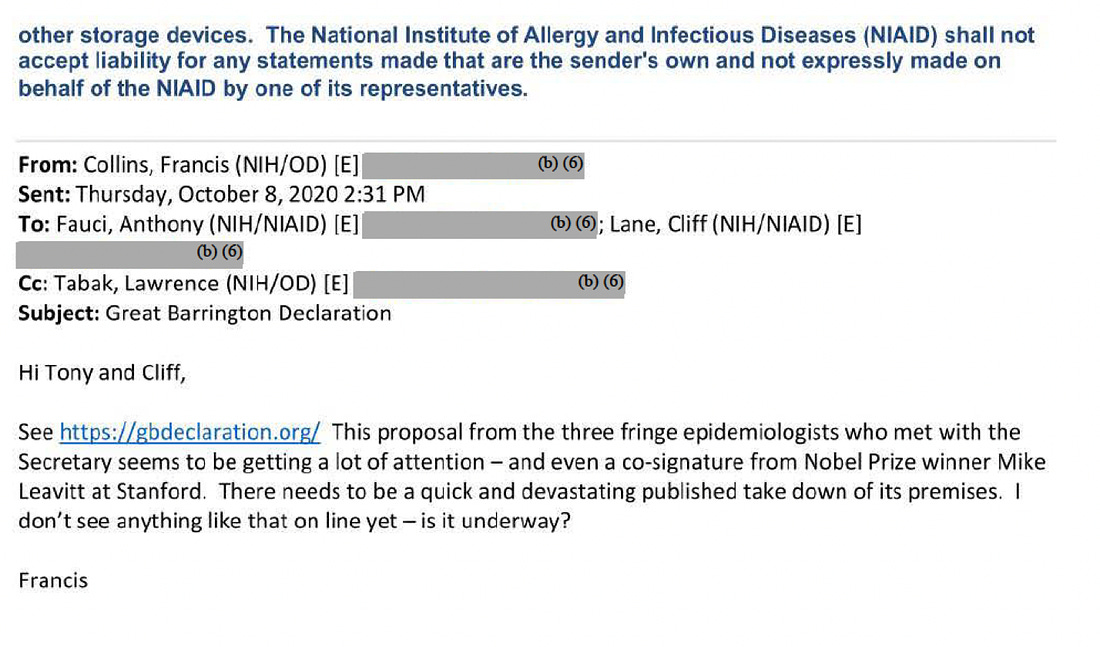
The three “fringe” epidemiologists referenced in the email were professors from Harvard, Oxford and Stanford (here, here, and here).
These three epidemiologists had launched the Great Barrington Declaration, which called for focused protection of high-risk individuals rather than blanket lockdowns. To date, tens of thousands of scientists and doctors have signed the declaration.
Collins apparently felt that he knew all he needed to know about lockdowns, and didn’t want to hear the opinions of other scientists or doctors.
The response to the above email from Fauci referenced a piece from WIRED as an example of the “quick and devastating published takedown” that Collins wanted.
Fauci’s behavior in response to the COVID pandemic has some striking similarities to how he handled the AIDS crisis; he has focused on vaccines or expensive drugs (like remdesivir) that would help make pharmaceuticals money, over other interventions like cheap health measures that people could take to improve their health outcomes, or generic drugs that are off patent (would not make Pharma any money) that could treat COVID.
His role in the Wuhan lab leak needs to be investigated. At the very least, we should all be asking why the NIH was trying to conceal any documents related to the lab leak; The Intercept had to sue for their release.
If even a fraction of this were true, it begs the question: how are we not hearing more about this in the media?
That gets into what’s wrong with our media.
Bonus: Explanations for why we are not hearing about this in the mediaThis section is a little different. It’s not here as part of the evidence for vaccine adverse events being underreported per say, but I thought I needed to address how it could be that we haven’t heard much about this from the media.
If Covid vaccines were actually harming and even killing significant numbers of people, how is it possible that this wouldn’t get covered in the media? This begs for some kind of explanation.
Censorship, and the merger of state, media, and tech
So much could be said about the amount of money pharmaceutical companies spend in advertising, but I suggest you listen to the aforementioned podcast with Dr. John Abramson, if you haven’t already. Here’s a summary.
......








