Moderators: Elvis, DrVolin, Jeff
![]() by alloneword » Thu Mar 26, 2020 2:13 pm
by alloneword » Thu Mar 26, 2020 2:13 pm

![]() by PufPuf93 » Thu Mar 26, 2020 2:44 pm
by PufPuf93 » Thu Mar 26, 2020 2:44 pm
Harvey » Thu Mar 26, 2020 6:11 am wrote:Love it, thanks Alloneword^
Thanks to Wombat^^ and to Jack, for his long piece half a dozen pages back (both being particularly memorable.) Mack was a bit of a shit (Kos certainly didn't deserve that) but his heart is always in the right place and as usual I don't disagree with much in what he's said. Disaster capitalism, war opportunism, confusionism and propaganda as usual, more so than usual.

![]() by JackRiddler » Thu Mar 26, 2020 3:07 pm
by JackRiddler » Thu Mar 26, 2020 3:07 pm
![]() by alloneword » Thu Mar 26, 2020 6:29 pm
by alloneword » Thu Mar 26, 2020 6:29 pm
Imperial College scientist who predicted 500K coronavirus deaths in UK revises to 20K or fewer
by Andrew Mark Miller
| March 26, 2020 11:59 AM
A scientist who warned that the coronavirus would kill 500,000 people in the United Kingdom has revised the estimate to roughly 20,000 people or fewer.
Scientist and Imperial College author Neil Ferguson said Wednesday that the coronavirus death toll is unlikely to exceed 20,000 and could be much lower, according to New Scientist. He added that he is “reasonably confident” that Britain’s health system can handle the burden of treating coronavirus patients.
“There will be some areas that are extremely stressed, but we are reasonably confident — which is all we can be at the current time — that at the national level we will be within capacity,” Ferguson said.
The Imperial College had previously warned of modeling that suggested over 500,000 would die from the virus.
“This is a remarkable turn from Neil Ferguson, who led the @imperialcollege authors who warned of 500,000 UK deaths - and who has now himself tested positive for #COVID,” former New York Times reporter Alex Berenson wrote on Twitter.
![]() by alloneword » Thu Mar 26, 2020 7:36 pm
by alloneword » Thu Mar 26, 2020 7:36 pm
![]() by DrEvil » Thu Mar 26, 2020 8:11 pm
by DrEvil » Thu Mar 26, 2020 8:11 pm
alloneword » Fri Mar 27, 2020 12:29 am wrote:Imperial College scientist who predicted 500K coronavirus deaths in UK revises to 20K or fewer
by Andrew Mark Miller
| March 26, 2020 11:59 AM
A scientist who warned that the coronavirus would kill 500,000 people in the United Kingdom has revised the estimate to roughly 20,000 people or fewer.
Scientist and Imperial College author Neil Ferguson said Wednesday that the coronavirus death toll is unlikely to exceed 20,000 and could be much lower, according to New Scientist. He added that he is “reasonably confident” that Britain’s health system can handle the burden of treating coronavirus patients.
“There will be some areas that are extremely stressed, but we are reasonably confident — which is all we can be at the current time — that at the national level we will be within capacity,” Ferguson said.
The Imperial College had previously warned of modeling that suggested over 500,000 would die from the virus.
“This is a remarkable turn from Neil Ferguson, who led the @imperialcollege authors who warned of 500,000 UK deaths - and who has now himself tested positive for #COVID,” former New York Times reporter Alex Berenson wrote on Twitter.
https://www.washingtonexaminer.com/news ... 0k-or-less
...snip...

![]() by Nordic » Thu Mar 26, 2020 9:31 pm
by Nordic » Thu Mar 26, 2020 9:31 pm
Enough people in money and power took it seriously enough to dump their stock. And anyone with a working brain knew it was coming and took it very seriously way the fuck before Tom fucking Hanks.
![]() by Wombaticus Rex » Thu Mar 26, 2020 9:34 pm
by Wombaticus Rex » Thu Mar 26, 2020 9:34 pm
1/4 - I think it would be helpful if I cleared up some confusion that has emerged in recent days. Some have interpreted my evidence to a UK parliamentary committee as indicating we have substantially revised our assessments of the potential mortality impact of COVID-19.
2/4 -This is not the case. Indeed, if anything, our latest estimates suggest that the virus is slightly more transmissible than we previously thought. Our lethality estimates remain unchanged.
3/4 - My evidence to Parliament referred to the deaths we assess might occur in the UK in the presence of the very intensive social distancing and other public health interventions now in place.
4/4 - Without those controls, our assessment remains that the UK would see the scale of deaths reported in our study (namely, up to approximately 500 thousand).
Is COVID-19 a global crisis? Certainly for people who can’t add.
I learned some powerful lessons from SARS in 2003. Maybe the most important one was how important it was to focus on what has happened rather than on what might happen. In other words: “Just the facts, ma’am."

![]() by Belligerent Savant » Thu Mar 26, 2020 10:26 pm
by Belligerent Savant » Thu Mar 26, 2020 10:26 pm
The global furor over the emerging coronavirus pandemic has masked one of the worst influenza seasons on record, government data show, particularly among children and young adults.
With flu season still winding down, at least 144 children younger than 18 have died, a toll topped only by the 2009 H1N1 pandemic since health authorities began tracking flu data in 2004.
So far this season, the U.S. Centers for Disease Control and Prevention has recorded 36 million flu cases in the U.S., with 370,000 hospitalizations and 22,000 deaths.
As of March 7, CDC reports, "hospitalization rates in children 0-4 years old and adults 18-49 years old are now the highest on record for these age groups, surpassing the rate reported during the 2009 H1N1 pandemic."
Despite the record numbers, influenza has all but been ignored, says Dr. Roger Klein, a molecular pathologist at Yale University. "There's been very little mention of it."
Flu experts say that's not surprising.
"Flu is an old enemy. We're kind of used to it," says Dr. William Schaffner, professor of preventive medicine and infectious diseases at the Vanderbilt University School of Medicine. "Coronavirus is new, mysterious, unknown. We didn't want it to come here, but it came and [with] a fatality rate among older people that is probably higher than flu. The entire human population is susceptible to this new virus, and it's working its way around the world. Who goes into shelter at home or lockdown for flu?"
While everyone (most everyone) is in a panic about the coronavirus, there should be a comparison with the annual flu. Statements that coronavirus is worse than the flu are simply not true. The following is from the Centers for Disease Control (CDC).While everyone is in a panic about the coronavirus (officially renamed COVID-19 by the World Health Organization), there’s an even deadlier virus many people are forgetting about: the flu.
Flu season is hitting its stride right now in the United States. So far, the CDC has estimated (based on weekly influenza surveillance data) that at least 12,000 people have died from influenza between Oct. 1, 2019, through Feb. 1, 2020.The CDC also estimates that up to 31 million Americans have caught the flu this season, with 210,000 to 370,000 flu sufferers hospitalized because of the virus.
“The current flu season has been difficult but it has not reached epidemic threshold,” infectious disease expert Amesh A. Adalja, MD, senior scholar at the John’s Hopkins Center for Health Security in Baltimore, said. “In the next couple of weeks, when more data is available, it will become clear just how severe the season was given that we had an initial dominance of influenza B and now dominance of influenza A H1N1.”
So how do these numbers compare to flu deaths in previous years? So far, it looks like the 2019-2020 death toll won’t be as high as it was in the 2017-2018 season, when 61,000 deaths were linked to the virus. However, it could equal or surpass the 2018-2019 season’s 34,200 flu-related deaths. Overall, the CDC estimates that 12,000 and 61,000 deaths annually since 2010 can be blamed on the flu. Globally, the World Health Organization (WHO) estimates that the flu kills 290,000 to 650,000 people per year.
The fact that people are more concerned about COVID-19 than the flu virus is no surprise, says Dr. Adalja. “Anytime there is a new emerging infectious disease that is shrouded in mystery with a lot of unknowns, it captivates people in a way that a regular virus that people deal with on a yearly basis won’t,” he says.

![]() by Wombaticus Rex » Thu Mar 26, 2020 10:58 pm
by Wombaticus Rex » Thu Mar 26, 2020 10:58 pm
Belligerent Savant » Thu Mar 26, 2020 9:26 pm wrote:Anyone here think COVID-19 will come close to those flu numbers? They sure as hell aren't remotely close, nor trending in that direction.
Belligerent Savant » Thu Mar 26, 2020 9:26 pm wrote:Yet, prior to March 1 (in the U.S., at least), we've heard nary a word from the media on the deaths caused by the FLU this season.
![]() by Belligerent Savant » Thu Mar 26, 2020 11:03 pm
by Belligerent Savant » Thu Mar 26, 2020 11:03 pm
![]() by Grizzly » Thu Mar 26, 2020 11:45 pm
by Grizzly » Thu Mar 26, 2020 11:45 pm

![]() by alloneword » Fri Mar 27, 2020 10:26 am
by alloneword » Fri Mar 27, 2020 10:26 am
In announcing the most far-reaching restrictions on personal freedom in the history of our nation, Boris Johnson resolutely followed the scientific advice that he had been given. The advisers to the government seem calm and collected, with a solid consensus among them. In the face of a new viral threat, with numbers of cases surging daily, I’m not sure that any prime minister would have acted very differently.
But I’d like to raise some perspectives that have hardly been aired in the past weeks, and which point to an interpretation of the figures rather different from that which the government is acting on. I’m a recently-retired Professor of Pathology and NHS consultant pathologist, and have spent most of my adult life in healthcare and science – fields which, all too often, are characterised by doubt rather than certainty. There is room for different interpretations of the current data. If some of these other interpretations are correct, or at least nearer to the truth, then conclusions about the actions required will change correspondingly.
The simplest way to judge whether we have an exceptionally lethal disease is to look at the death rates. Are more people dying than we would expect to die anyway in a given week or month? Statistically, we would expect about 51,000 to die in Britain this month. At the time of writing, 422 deaths are linked to Covid-19 — so 0.8 per cent of that expected total. On a global basis, we’d expect 14 million to die over the first three months of the year. The world’s 18,944 coronavirus deaths represent 0.14 per cent of that total. These figures might shoot up but they are, right now, lower than other infectious diseases that we live with (such as flu). Not figures that would, in and of themselves, cause drastic global reactions.
Initial reported figures from China and Italy suggested a death rate of 5 per cent to 15 per cent, similar to Spanish flu. Given that cases were increasing exponentially, this raised the prospect of death rates that no healthcare system in the world would be able to cope with. The need to avoid this scenario is the justification for measures being implemented: the Spanish flu is believed to have infected about one in four of the world’s population between 1918 and 1920, or roughly 500 million people with 50 million deaths. We developed pandemic emergency plans, ready to snap into action in case this happened again.
At the time of writing, the UK’s 422 deaths and 8,077 known cases give an apparent death rate of 5 per cent. This is often cited as a cause for concern, contrasted with the mortality rate of seasonal flu, which is estimated at about 0.1 per cent. But we ought to look very carefully at the data. Are these figures really comparable?
Most of the UK testing has been in hospitals, where there is a high concentration of patients susceptible to the effects of any infection. As anyone who has worked with sick people will know, any testing regime that is based only in hospitals will over-estimate the virulence of an infection. Also, we’re only dealing with those Covid-19 cases that have made people sick enough or worried enough to get tested. There will be many more unaware that they have the virus, with either no symptoms, or mild ones.
That’s why, when Britain had 590 diagnosed cases, Sir Patrick Vallance, the government’s chief scientific adviser, suggested that the real figure was probably between 5,000 and 10,000 cases, ten to 20 times higher. If he’s right, the headline death rate due to this virus is likely to be ten to 20 times lower, say 0.25 per cent to 0.5 per cent. That puts the Covid-19 mortality rate in the range associated with infections like flu.
But there’s another, potentially even more serious problem: the way that deaths are recorded. If someone dies of a respiratory infection in the UK, the specific cause of the infection is not usually recorded, unless the illness is a rare ‘notifiable disease’. So the vast majority of respiratory deaths in the UK are recorded as bronchopneumonia, pneumonia, old age or a similar designation. We don’t really test for flu, or other seasonal infections. If the patient has, say, cancer, motor neurone disease or another serious disease, this will be recorded as the cause of death, even if the final illness was a respiratory infection. This means UK certifications normally under-record deaths due to respiratory infections.
Now look at what has happened since the emergence of Covid-19. The list of notifiable diseases has been updated. This list — as well as containing smallpox (which has been extinct for many years) and conditions such as anthrax, brucellosis, plague and rabies (which most UK doctors will never see in their entire careers) — has now been amended to include Covid-19. But not flu. That means every positive test for Covid-19 must be notified, in a way that it just would not be for flu or most other infections.
In the current climate, anyone with a positive test for Covid-19 will certainly be known to clinical staff looking after them: if any of these patients dies, staff will have to record the Covid-19 designation on the death certificate — contrary to usual practice for most infections of this kind. There is a big difference between Covid-19 causing death, and Covid-19 being found in someone who died of other causes. Making Covid-19 notifiable might give the appearance of it causing increasing numbers of deaths, whether this is true or not. It might appear far more of a killer than flu, simply because of the way deaths are recorded.
If we take drastic measures to reduce the incidence of Covid-19, it follows that the deaths will also go down. We risk being convinced that we have averted something that was never really going to be as severe as we feared. This unusual way of reporting Covid-19 deaths explains the clear finding that most of its victims have underlying conditions — and would normally be susceptible to other seasonal viruses, which are virtually never recorded as a specific cause of death.
Let us also consider the Covid-19 graphs, showing an exponential rise in cases — and deaths. They can look alarming. But if we tracked flu or other seasonal viruses in the same way, we would also see an exponential increase. We would also see some countries behind others, and striking fatality rates. The United States Centers for Disease Control, for example, publishes weekly estimates of flu cases. The latest figures show that since September, flu has infected 38 million Americans, hospitalised 390,000 and killed 23,000. This does not cause public alarm because flu is familiar.
The data on Covid-19 differs wildly from country to country. Look at the figures for Italy and Germany. At the time of writing, Italy has 69,176 recorded cases and 6,820 deaths, a rate of 9.9 per cent. Germany has 32,986 cases and 157 deaths, a rate of 0.5 per cent. Do we think that the strain of virus is so different in these nearby countries as to virtually represent different diseases? Or that the populations are so different in their susceptibility to the virus that the death rate can vary more than twentyfold? If not, we ought to suspect systematic error, that the Covid-19 data we are seeing from different countries is not directly comparable.
Look at other rates: Spain 7.1 per cent, US 1.3 per cent, Switzerland 1.3 per cent, France 4.3 per cent, South Korea 1.3 per cent, Iran 7.8 per cent. We may very well be comparing apples with oranges. Recording cases where there was a positive test for the virus is a very different thing to recording the virus as the main cause of death.
Early evidence from Iceland, a country with a very strong organisation for wide testing within the population, suggests that as many as 50 per cent of infections are almost completely asymptomatic. Most of the rest are relatively minor. In fact, Iceland’s figures, 648 cases and two attributed deaths, give a death rate of 0.3 per cent. As population testing becomes more widespread elsewhere in the world, we will find a greater and greater proportion of cases where infections have already occurred and caused only mild effects. In fact, as time goes on, this will become generally truer too, because most infections tend to decrease in virulence as an epidemic progresses.
One pretty clear indicator is death. If a new infection is causing many extra people to die (as opposed to an infection present in people who would have died anyway) then it will cause an increase in the overall death rate. But we have yet to see any statistical evidence for excess deaths, in any part of the world.
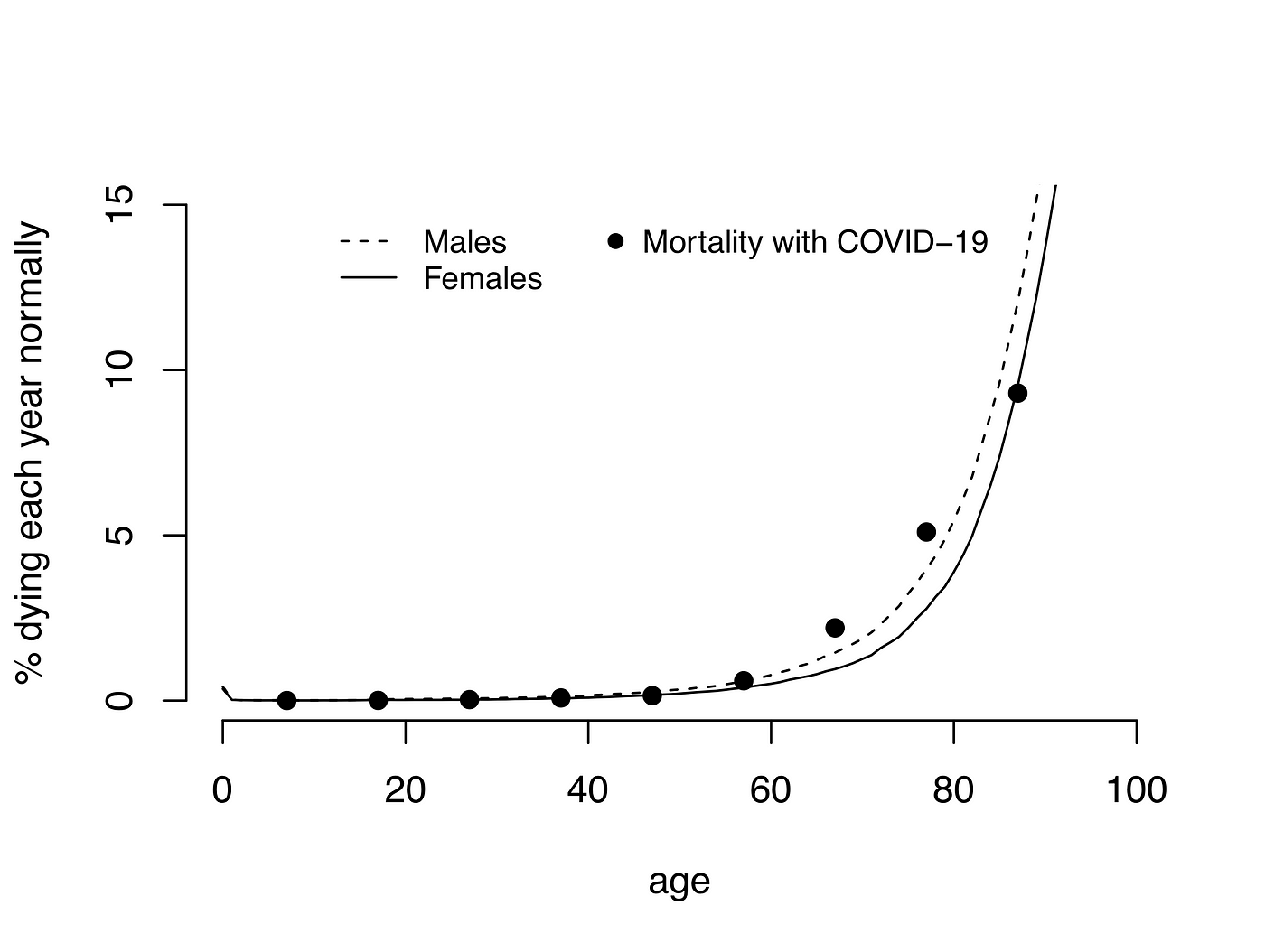
Covid-19 can clearly cause serious respiratory tract compromise in some patients, especially those with chest issues, and in smokers. The elderly are probably more at risk, as they are for infections of any kind. The average age of those dying in Italy is 78.5 years, with almost nine in ten fatalities among the over-70s. The life expectancy in Italy — that is, the number of years you can expect to live to from birth, all things being equal — is 82.5 years. But all things are not equal when a new seasonal virus goes around.
It certainly seems reasonable, now, that a degree of social distancing should be maintained for a while, especially for the elderly and the immune-suppressed. But when drastic measures are introduced, they should be based on clear evidence. In the case of Covid-19, the evidence is not clear. The UK’s lockdown has been informed by modelling of what might happen. More needs to be known about these models. Do they correct for age, pre-existing conditions, changing virulence, the effects of death certification and other factors? Tweak any of these assumptions and the outcome (and predicted death toll) can change radically.
Much of the response to Covid-19 seems explained by the fact that we are watching this virus in a way that no virus has been watched before. The scenes from the Italian hospitals have been shocking, and make for grim television. But television is not science.
Clearly, the various lockdowns will slow the spread of Covid-19 so there will be fewer cases. When we relax the measures, there will be more cases again. But this need not be a reason to keep the lockdown: the spread of cases is only something to fear if we are dealing with an unusually lethal virus. That’s why the way we record data will be hugely important. Unless we tighten criteria for recording death due only to the virus (as opposed to it being present in those who died from other conditions), the official figures may show a lot more deaths apparently caused by the virus than is actually the case. What then? How do we measure the health consequences of taking people’s lives, jobs, leisure and purpose away from them to protect them from an anticipated threat? Which causes least harm?
The moral debate is not lives vs money. It is lives vs lives. It will take months, perhaps years, if ever, before we can assess the wider implications of what we are doing. The damage to children’s education, the excess suicides, the increase in mental health problems, the taking away of resources from other health problems that we were dealing with effectively. Those who need medical help now but won’t seek it, or might not be offered it. And what about the effects on food production and global commerce, that will have unquantifiable consequences for people of all ages, perhaps especially in developing economies?
Governments everywhere say they are responding to the science. The policies in the UK are not the government’s fault. They are trying to act responsibly based on the scientific advice given. But governments must remember that rushed science is almost always bad science. We have decided on policies of extraordinary magnitude without concrete evidence of excess harm already occurring, and without proper scrutiny of the science used to justify them.
In the next few days and weeks, we must continue to look critically and dispassionately at the Covid-19 evidence as it comes in. Above all else, we must keep an open mind — and look for what is, not for what we fear might be.
John Lee is a recently retired professor of pathology and a former NHS consultant pathologist.
![]() by Iamwhomiam » Fri Mar 27, 2020 11:17 am
by Iamwhomiam » Fri Mar 27, 2020 11:17 am
In announcing the most far-reaching restrictions on personal freedom in the history of our nation, Boris Johnson resolutely followed the scientific advice that he had been given. The advisers to the government seem calm and collected, with a solid consensus among them. In the face of a new viral threat, with numbers of cases surging daily, I’m not sure that any prime minister would have acted very differently.
![]() by Wombaticus Rex » Fri Mar 27, 2020 11:50 am
by Wombaticus Rex » Fri Mar 27, 2020 11:50 am
Iamwhomiam » Fri Mar 27, 2020 10:17 am wrote:I'm not sure if Rex would agree, but I believe we're at least one month away from its peak in NYS.
Users browsing this forum: No registered users and 6 guests
