https://twitter.com/search?q=%23VaccinO ... head_click
Moderators: Elvis, DrVolin, Jeff

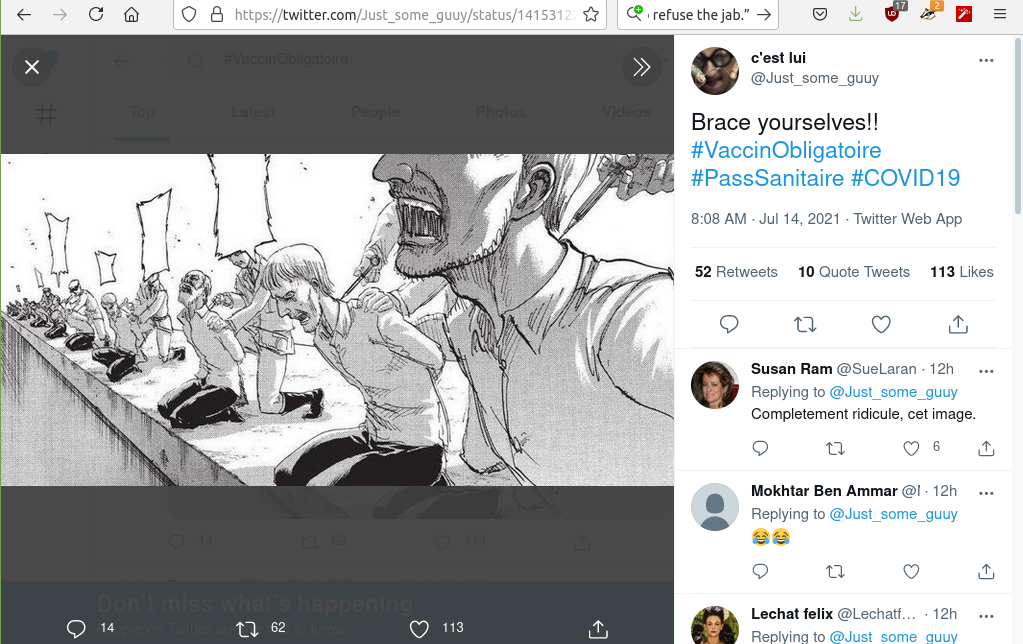
The real photos from the protests are bad enough and condemn the French state. Creating imaginary images of something that did not happen has the opposite effect.Grizzly » Wed Jul 14, 2021 11:17 pm wrote:Covid vaccination rioting in France?
https://twitter.com/search?q=%23VaccinO ... head_click
God, you and other's here are a snobby pretentious bunch....The real photos from the protests are bad enough and condemn the French state. Creating imaginary images of something that did not happen has the opposite effect.

That one? Not at all. Sober little cartoon, not trying to overheat emotions on an irrational plane, not exaggerating current reality, making an important point clearly. Sure, I'd probably have "Capitalist System" doing the pushing, of which USG is a part, but six of one, half dozen of the other.Grizzly » Fri Jul 16, 2021 5:46 am wrote:jr
God, you and other's here are a snobby pretentious bunch....The real photos from the protests are bad enough and condemn the French state. Creating imaginary images of something that did not happen has the opposite effect.
Here's another subjective view that you all will prolly snub too...

Is it really necessary to inform people that healthy living is good for them? Pretty self-evident. If they're not doing it already it's not because they don't know any better.Karmamatterz » Fri Jul 16, 2021 8:13 pm wrote:
...
I'll repeat myself again: How many ( and how often ) were elected officials, bureaucrats, big pharma shills and media talking botheads suggesting to the citizenry that they eat healthy, exercise, get outside for sunshine and fresh air? Did they do this daily? Weekly? How about almost never.
How many other medical treatments have been shoved down our throats like these experimental vaccines? None!
...
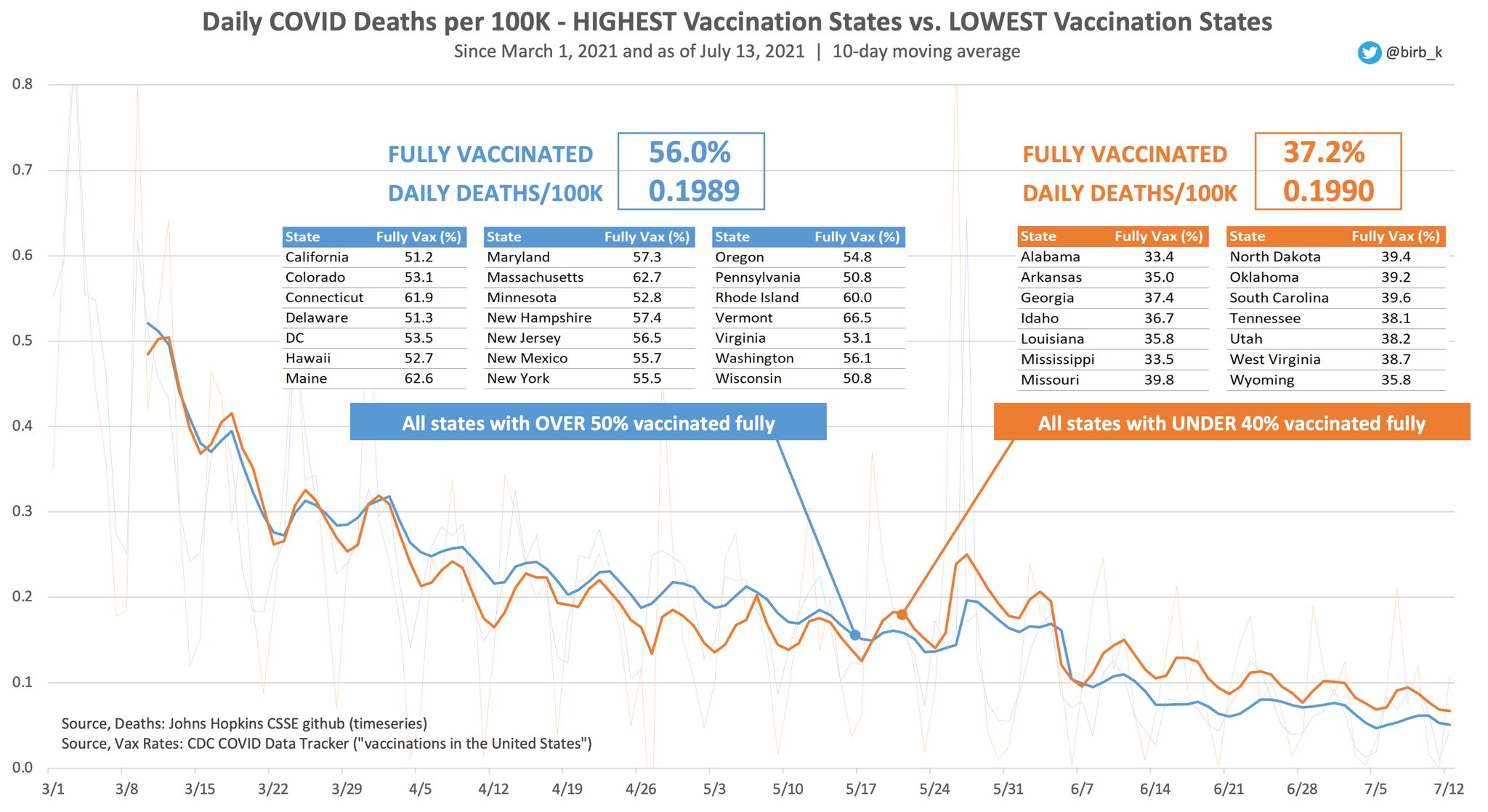
There's a reason death rates started dropping before the vaccines came along, and that's because they figured out how to treat it better, but they don't shove treatments down your throat until you need them, at which point you're probably already at the hospital. The whole point of vaccines is to stop you from needing treatment at all.How many other medical treatments have been shoved down our throats like these experimental vaccines? None!

DrEvil » Fri Jul 16, 2021 6:55 pm wrote:Is it really necessary to inform people that healthy living is good for them? Pretty self-evident. If they're not doing it already it's not because they don't know any better.Karmamatterz » Fri Jul 16, 2021 8:13 pm wrote:
...
I'll repeat myself again: How many ( and how often ) were elected officials, bureaucrats, big pharma shills and media talking botheads suggesting to the citizenry that they eat healthy, exercise, get outside for sunshine and fresh air? Did they do this daily? Weekly? How about almost never.
How many other medical treatments have been shoved down our throats like these experimental vaccines? None!
...
There's a reason death rates started dropping before the vaccines came along, and that's because they figured out how to treat it better, but they don't shove treatments down your throat until you need them, at which point you're probably already at the hospital. The whole point of vaccines is to stop you from needing treatment at all.How many other medical treatments have been shoved down our throats like these experimental vaccines? None!
Remember, the formal literature from each shot manufacturer never claim to immunize, only lessen symptoms, and even that is no guarantee.

Misleading clinical evidence and systematic reviews on ivermectin for COVID-19
Since WHO declared the COVID-19 as a pandemic,1 2 healthcare systems all over the world have focused their efforts on limiting the spread of SARS-CoV-2, and despite the ceaseless development of strategies to struggle with the impact of COVID-19, there is no sign of let-up. And the stress and overburden elicited by the pandemic—especially in vulnerable or marginalised populations—remain unstoppable, while the possibility of massive vaccination gives hope for a respite.3 4 Beyond public health interventions, several drugs have been considered for the treatment of SARS-CoV-2 infection,5 which triggers severe respiratory symptoms and critical illness in approximately 5%–20% of patients, with intensive care requirements and high mortality.6–10 In this article, we appraise and debate about the available evidence regarding the role of ivermectin for COVID-19.
Randomised Evaluation of COVID-19 Therapy (RECOVERY) trial results have had a critical role establishing the most useful pharmacological interventions in COVID-19 critical care, such as dexamethasone.11 However, despite the development of new therapies and the attempts for implementing repurposed drugs (because of their potential immunomodulator or antiviral effects), no reliable specific therapy has been identified yet. Azithromycin, chloroquine and hydroxychloroquine are some of those drugs, whose adverse effects and/or concerns about efficacy on COVID-19 treatment12 have determined its deimplementation by different agencies and regulatory authorities.13–15 And despite the wide dissemination of these recommendations, paradoxically, its adherence in both high-income, and middle-income and low-income countries has been hindered not only by the COVID-19 social media infodemic, but also by authorities.16
Ivermectin is a broad-spectrum antiparasitic agent approved by the Food and Drug Administration (FDA) of the USA proved to be safe at the conventional dose of ≤200 µg/kg, although severe adverse effects ranging from ataxia to seizures have occasionally been reported.5 And due to its in vitro antiviral activity against a broad range of viruses, it has been used off-label for the treatment of some viral diseases.13 17
In a vertiginous search for COVID-19 treatments, Caly et al conducted an in vitro exploration that showed ivermectin’s inhibitor role on the replication of the SARS-CoV-2 virus,17 18 among few other in silico and in vitro results suggesting the same.19–21 Thus, a considerable amount of preprints and protocol records quickly appeared, reporting the clinical efficacy of ivermectin in standard doses for COVID-19. The dissemination of these results caused confusion, and the general population and some clinicians endorsed the use of ivermectin, especially in Latin America.22 However, in a matter of days since the publication of Caly et al17 and its repercussions, a general publication from the Pan American Health Organization (PAHO) stated that “…ivermectin is incorrectly being used for the treatment of COVID-19, without any scientific evidence of its efficacy and safety for the treatment of this disease.”23
An important controversial point to consider in any rationale is the 5 µM required concentration to reach the anti-SARS-CoV-2 action of ivermectin observed in vitro,17 which is much higher than 0.28 µM, the maximum reported plasma concentration achieved in vivo with a dose of approximately 1700 µg/kg (about nine times the FDA-approved dosification).24 25 In this sense, basic fundamentals for assessing ivermectin in COVID-19 at a clinical level appear to be insufficient. Among other reasons, we believe this might have led WHO to exclude ivermectin from its Solidarity Trial for repurposed drugs for COVID-19,12 which raises questions about the pertinence of conducting clinical studies on ivermectin.
Nevertheless, assessments of ivermectin as prophylaxis or treatment for mild to severe COVID-19 continue being published in preprints26 27 and protocol repositories,28 29 which do not follow the recommended process to ensure quality standards in publications; whereas peer-reviewed reports (both observational and experimental studies) are slowly emerging, yet methodologically limited by heterogeneity in population receiving ivermectin, dosis applied and uncontrolled cointerventions.28–30 Similarly, other studies that can be rapidly retrieved in ClinicalTrials.gov, medRxiv and MEDLINE make up a quite heterogeneous body of evidence31–33 (including ivermectin as intervention, but with different underlying clinical questions), among other issues that do not contribute to the certainty of evidence—according to the systematic reviews that we comment on below.
Up to February 2021, the PAHO identified twenty two ivermectin randomised clinical trials through a rapid review of current available literature.34 There is considerable heterogeneity in the population receiving ivermectin, with studies administering it to family contacts of confirmed COVID-19 cases as a prophylactic measure29 and other studies using ivermectin for treatment of mild and moderate infected cases28 or even severe hospitalised patients.30 Applied dosis and outcomes of interest were also highly variable. Additionally, patients also received various cointerventions, and control groups received different kinds of comparators ranging from placebo or no intervention to standard care or even hydroxychloroquine. The authors claim that pooled estimates suggest beneficial effects with ivermectin, but the certainty of the evidence was very low due to high risk of bias and small number of events throughout the included studies. Most study results have been made publicly available as preprints or unpublished, with no peer review or formal editorial process. Others incorporated their results only in the clinical trial register, but nearly half of these randomised clinical trials had not been registered. Registering clinical trials before they begin and making results available fulfils a large number of purposes, like reducing publication and selective outcome reporting biases, promoting more efficient allocation of research funds and facilitating evidence syntheses that will inform stakeholders and decision-makers in the future.
A recently published systematic review and network meta-analysis35 compared the efficacy and safety of pharmacological interventions for COVID-19 in hospitalised patients. It included 110 studies (78 published and 38 unpublished) with 40 randomised clinical trials and 70 observational studies. Based on observational data, they found that high-dose intravenous immunoglobulin, ivermectin and tocilizumab were associated with reduced mortality rate in critically ill patients. None of the analysed drugs was significantly associated with increased non-cardiac serious adverse events compared with standard care, but the overall certainty of the evidence was very low in all outcomes and reduced the ability for recommendation.
Different websites (such as https://ivmmeta.com/, https://c19ivermectin.com/, https://tratamientotemprano.org/estudios-ivermectina/, among others) have conducted meta-analyses with ivermectin studies, showing unpublished colourful forest plots which rapidly gained public acknowledgement and were disseminated via social media, without following any methodological or report guidelines. These websites do not include protocol registration with methods, search strategies, inclusion criteria, quality assessment of the included studies nor the certainty of the evidence of the pooled estimates. Prospective registration of systematic reviews with or without meta-analysis protocols is a key feature for providing transparency in the review process and ensuring protection against reporting biases, by revealing differences between the methods or outcomes reported in the published review and those planned in the registered protocol. These websites show pooled estimates suggesting significant benefits with ivermectin, which has resulted in confusion for clinicians, patients and even decision-makers. This is usually a problem when performing meta-analyses which are not based in rigorous systematic reviews, often leading to spread spurious or fallacious findings.36
Concluding, research related to ivermectin in COVID-19 has serious methodological limitations resulting in very low certainty of the evidence, and continues to grow.37–39 The use of ivermectin, among others repurposed drugs for prophylaxis or treatment for COVID-19, should be done based on trustable evidence, without conflicts of interest, with proven safety and efficacy in patient-consented, ethically approved, randomised clinical trials.
This opinion piece, to be clear, does not indicate Ivermectin is NOT effective.mentalgongfu2 » Sat Jul 17, 2021 7:15 am wrote:https://ebm.bmj.com/content/early/2021/ ... 021-111678
Misleading clinical evidence and systematic reviews on ivermectin for COVID-19
...
Belligerent Savant » Wed Dec 09, 2020 9:38 pm wrote:.
More on ivermectin, referenced above.
https://www.sciencedirect.com/science/a ... 4220302011
The FDA-approved drug ivermectin inhibits the replication of SARS-CoV-2 in vitro
Highlights
•
Ivermectin is an inhibitor of the COVID-19 causative virus (SARS-CoV-2) in vitro.
•
A single treatment able to effect ~5000-fold reduction in virus at 48 h in cell culture.
•
Ivermectin is FDA-approved for parasitic infections, and therefore has a potential for repurposing.
•
Ivermectin is widely available, due to its inclusion on the WHO model list of essential medicines.
Abstract
Although several clinical trials are now underway to test possible therapies, the worldwide response to the COVID-19 outbreak has been largely limited to monitoring/containment. We report here that Ivermectin, an FDA-approved anti-parasitic previously shown to have broad-spectrum anti-viral activity in vitro, is an inhibitor of the causative virus (SARS-CoV-2), with a single addition to Vero-hSLAM cells 2 h post infection with SARS-CoV-2 able to effect ~5000-fold reduction in viral RNA at 48 h. Ivermectin therefore warrants further investigation for possible benefits in humans.
Joint Statement of the FLCCC Alliance and British Ivermectin Recommendation Development Group on Retraction of Early Research on Ivermectin
A reexamination of the data without the earlier research continues to prove that ivermectin is effective in preventing and treating COVID-19
Newswise — WASHINGTON, D.C. and BATH, SOMERSET, U.K. – The Front Line COVID-19 Critical Care Alliance (FLCCC), a group of highly published, world-renowned critical care physicians and scholars, and the British Ivermectin Recommendation Development Group (BIRD), a U.K. based group of medical and scientific experts from over 15 countries, are concerned over the misrepresentation of science in the recent article published in the Guardian regarding the withdrawal of Professor Emeritus Ahmed Elgazzar’s study into ivermectin that was first posted December 16, 2020.
Contrary to the voices quoted in the article, there is no scientific basis to state that the removal of one study from meta-analyses would ‘reverse results.’ Worryingly, this article’s insinuation is reported as if it is fact.
According to the most recent analyses by BIRD, excluding the Elgazzar data from the cited meta-analyses by Bryant and Hill does not change the conclusions of these reviews, with the findings still clearly favouring ivermectin for both prevention and treatment.
This article raise questions of journalistic integrity and we invite the Guardian to make appropriate corrections to the reporting and properly check the veracity of their claims.
“This is not just about correcting facts but about people’s lives,” said Dr. Tess Lawrie, director of the Evidence-Based Medicine Consultancy and organizer of the BIRD group. “Ivermectin is already in use around the world and can reach the poorest people long before other expensive COVID treatments will ever get to them. Ivermectin has an ever-increasing evidence base that shows that it works –even the prestigious Institute Pasteur in France has confirmed that the evidence is sound.”
“When we examine the extensive evidence on ivermectin as a treatment for COVID-19 without this latest study, we still see a significant reduction in the spread of COVID-19 as well as a reduction in hospitalizations and death,” said Dr. Pierre Kory, president and chief medical officer of the FLCCC. “All science needs to be scrutinized. As some of the most published researchers in our fields, we are used to having our work examined by others. I hope that Dr. Elgazzar’s work will be impartially judged and any errors that might be found are corrected.”
About the Front Line COVID-19 Critical Care Alliance
The FLCCC Alliance was organized in March 2020 by a group of highly published, world renowned Critical Care physician/scholars – with the academic support of allied physicians from around the world – to research and develop lifesaving protocols for the prevention and treatment of COVID-19 in all stages of illness. Their MATH+ Hospital Treatment Protocol, introduced in March 2020, has saved thousands of patients who were critically ill with COVID-19. Now, the FLCCC’s new I-Mask+ Prophylaxis and Early At-Home Outpatient Treatment Protocol with Ivermectin has been released – and is a potential solution to the global pandemic.
For more information: http://www.FLCCC.net
About the BIRD group
Convened by The Evidenced-Based Medical Consultancy (E-BMC) in Bath, United Kingdom, the BIRD meeting was assembled according to the World Health Organization Handbook of Guideline Development to review the latest science on the safety and efficacy of Ivermectin for the treatment and prevention of COVID-19. The expert panel included medical and scientific experts from 16 countries, including Argentina, Australia, Belgium, Canada, France, Hungary, India, Ireland, Japan, Peru, Nigeria, South Africa, Philippines, United States, United Kingdom

https://twitter.com/dockaurG/status/141 ... 54240?s=20Kulvinder Kaur MD
@dockaurG
·
Statement: pre-existing cross-reactive and post-infectious Tcell immunity to SARSCoV2 are more robust, broad and long-lasting than vaccine-acquired SARSCoV2 immunity
Question: please share & cite any published peer-reviewed scientific evidence that exists refuting this statement
@sincoscossin
·
Replying to
@dockaurG
This paper shows that people who recovered from SARS 17 years ago also had cross-immunity against COVID. This indicates that T-cell immunity works for a long time and is resistant to mutation.
https://www.nature.com/articles/s41586-020-2550-z