Variant Roulette (Evolution and Immunity Escape) Part 2Multiple recent papers have emerged that relate to the debate over whether vaccinated or unvaccinated people drive the emergence of SARS-CoV-2 variants since I wrote my first article on the topic. Let's take a look at what they tell us, and how vaccine partisans are misinterpreting them as publicly as possible.
A Computer ModelOn July 30, Rella et al reported in their paper Rates of SARS-CoV-2 transmission and vaccination impact the fate of vaccine-resistant strains on the results of computer simulations testing for variant emergence during the ups-and-downs of seasonal infection waves. From the abstract:
As expected, we found that a fast rate of vaccination decreases the probability of emergence of a resistant strain. Counterintuitively, when a relaxation of non-pharmaceutical interventions happened at a time when most individuals of the population have already been vaccinated the probability of emergence of a resistant strain was greatly increased. Consequently, we show that a period of transmission reduction close to the end of the vaccination campaign can substantially reduce the probability of resistant strain establishment.
As much as I dislike lockdowns and social distance and feel certain that the vast expansion of global food insecurity that resulted from those policies are likely to kill far more people (likely several times as many) than 20 months of COVID has, I can see the logic in avoiding indoor crowds this Winter. Just remember that you need to get outdoors when possible and almost no spread occurs outdoors. Wear your mittens.
More to the point, the Rella research team focused their modeling specifically on what they called "vaccine-resistant strains". Is this the right logic?
Those who claim the sloganesque "Unvaccinated are Variant Factories" would claim that vaccine-resistent strains are a subset of Variants of Interest. While they're not wrong, technically, let us remind ourselves that the Variants of Interest never seemed to emerge until vaccine trials were held, then emerged in the vicinities of where those trials were held. Also, the Variants of Interest strongly display the quality of escape from antibody classes:

While my own framing of the multiply-conditional problem of finding the probability that variants emerged from the vaccinated differs from that of the Rella team (that would take work that isn't at the top of my current priority list), I appreciate their approach and would now look for a way to incorporate it into my own model. And I'll be glad to piggy-back off of some of their work if I find the time to follow through with computations. And while I haven't performed those calculations, my belief is strongly that either there is >99.9% chance the variants are driven primarily by the vaccinated or a >99.9% chance that the variants are driven primarily by the unvaccinated. And given conditions such as when and where the variants emerged...I'll throw my wager on those receiving COVID-19 vaccines being the source...of...variants that fall into the category of vaccine-resistant strains.
The other side of the argument seems to have a steep uphill climb, and I've so far not talked to anyone in genetics who feels otherwise. The closest thing to that was an email exchange with Biostatistics Professor Jeffrey Morris, who began with the position, "All of these variants were around before vaccination started so, if vaccination produces any variants, they haven’t appeared yet." After I explained his mistake, he shifted to,
But vaccine trials involve thousands of individuals in a population of many millions.
There is no conceivable way for a few thousand vaccinated to drive the evolution of new variants.
But this takes no conditional into account. While geography is certainly not the most restrictive conditional (after all, we're talking about...vaccine-resistant variants as per antibody escape, not T cell or PK cell escape), this response disrespects the coincidence factor. Take the individual probability coincidence factor to the fourth power and we get something like a black swan. I politely offered to walk through the math, but he settled with, "I don’t need someone to walk me through the math; I am a Biostatistics professor." A few fruitless emails later, he produced no math at all.
I'm guessing he doesn't do work in genetics, but he might be the one person I've encountered with any computational genetics background sticking to the narrative. It is what it is, I guess.
Entertainingly, even CNN promoted the Rella paper, which may serve as a hedge to their participation in the "unvaccinated are variant factories" campaign.
The "Two Highly-Effective mRNA Vaccines" PaperThe bias in the title alone of Puranik et al's paper forces my eyes to roll, and not a little.
Reading the Competing Interests Statement gave me a rash.
AP, PJL, ES, MJN, JC, AJV, and VS are employees of nference and have financial interests in the company. nference is collaborating with Moderna, Pfizer, Janssen, and other bio-pharmaceutical companies on data science initiatives unrelated to this study. These collaborations had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. JCO receives personal fees from Elsevier and Bates College, and receives small grants from nference, Inc, outside the submitted work. ADB is supported by grants from NIAID (grants AI110173 and AI120698), Amfar (#109593), and Mayo Clinic (HH Shieck Khalifa Bib Zayed Al-Nahyan Named Professorship of Infectious Diseases). ADB is a paid consultant for Abbvie, Gilead, Freedom Tunnel, Pinetree therapeutics Primmune, Immunome and Flambeau Diagnostics, is a paid member of the DSMB for Corvus Pharmaceuticals, Equilium, and Excision Biotherapeutics, has received fees for speaking for Reach MD and Medscape, owns equity for scientific advisory work in Zentalis and nference, and is founder and President of Splissen Therapeutics. MDS received grant funding from Pfizer via Duke University for a vaccine side effect registry. JH, JCO, AV, MDS and ADB are employees of the Mayo Clinic. The Mayo Clinic may stand to gain financially from the successful outcome of the research. This research has been reviewed by the Mayo Clinic Conflict of Interest Review Board and is being conducted in compliance with Mayo Clinic Conflict of Interest policies.
The paper found a [much] lower efficacy reduction than is being seen in Israel for Pfizer's vaccine, or in the UK where both mRNA vaccines are in use. But I'm not going to go much further than that because I doubt many serious people will take this particularly seriously, except as biased and conflicted secondary evidence of efficacy against variants that is contradicted by that from other nations.
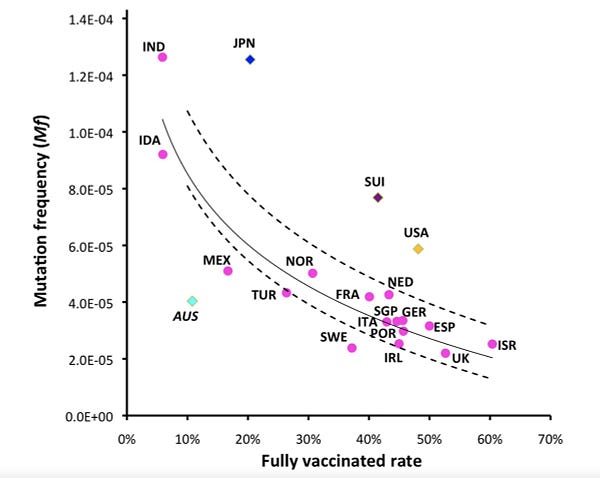
The Mutation Frequency PaperThree days ago Yeh and Contreras posted this preprint on medRxiv entitled Full vaccination suppresses SARS-CoV-2 delta variant mutation frequency. The abstract goes a step further, claiming this is the "first evidence that full vaccination against COVID-19 suppresses emergent mutations of SARS-CoV-2 delta variants". The problem is that this is a plainly incorrect interpretation of the results. While this paper isn't Lyu and Wehby absurd, it almost appears (to me) designed to mislead.
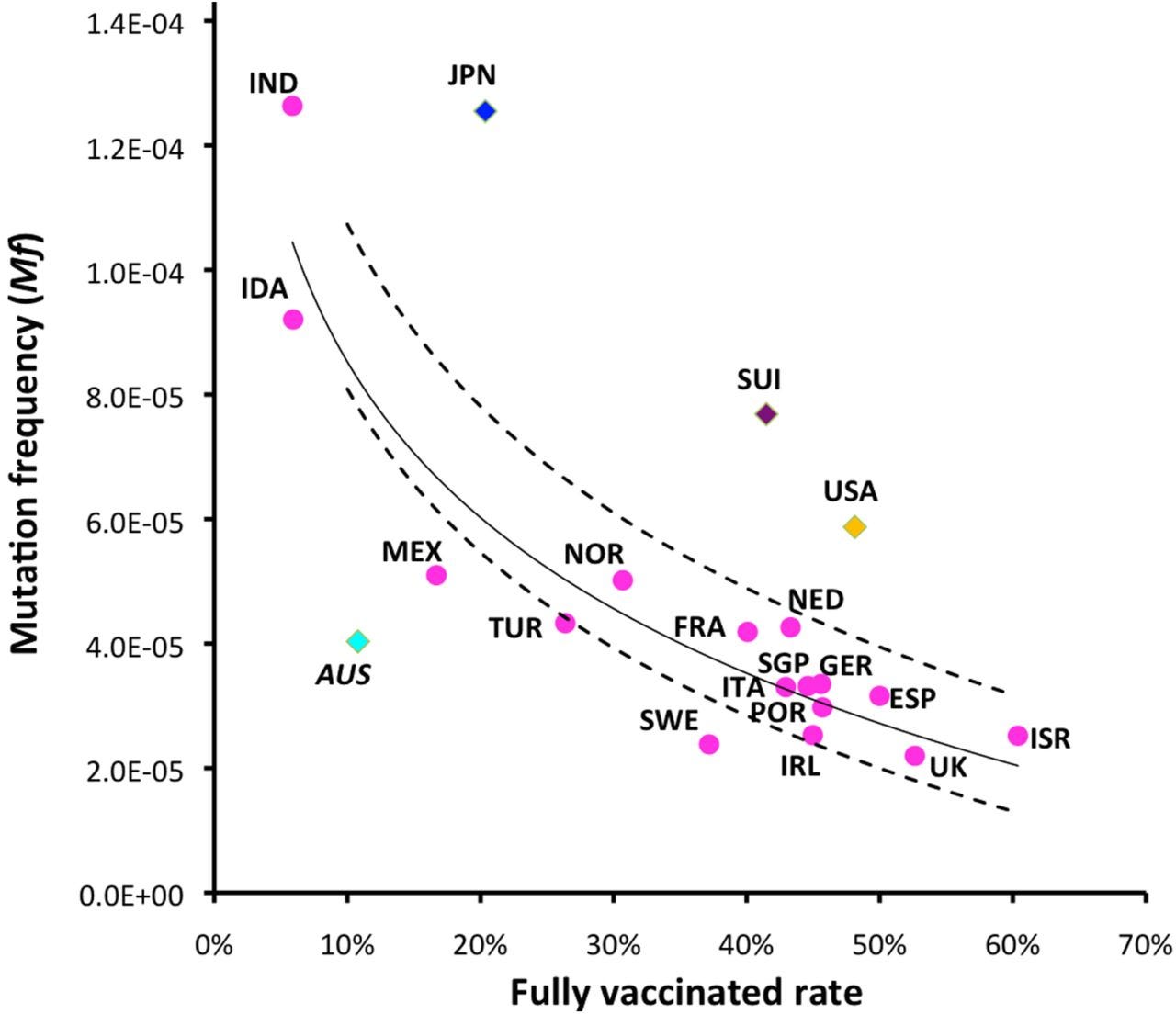
Before we move any further, we need to discuss one term defined in the paper, and another one which is not. For many readers unfamiliar with statistical genetics, the distinction will help to disambiguate between a correct understanding of the results of this graph, and an intuitive but false one.
Mutation frequency. Simply put, mutation frequency is the measured frequency of mutations (as they exist) in a population. A low mutation frequency represents a population with sequences that are highly similar, while a high mutation frequency represents a population with sequences that are less similar to each other.
Mutation rate. The mutation rate is the measured frequency of mutations over time. The higher the mutation rate, the more likely that the "offspring" of a virus differ (at any particular location or base pair) from the immediate progenitor (or per time/ancestral distance from any progenitor assuming nothing like a speciation event).
So, the mutation rate tells us (technically, this can be defined in context, but usually for a virus…) how many single nucleotide polymorphisms (SNPs, like "snips") we expect to see from one viral generation to the next. But the mutation frequency measures the abundance of SNPs relative to the virions in a generational pool. What we see in the graph above is that
greater vaccination results in greater selection pressure to eliminate those virions least like the others.
So, which virions do you imagine are being selected for in a highly vaccinated pool?
I'll give you one guess, and it's not the virions most easily neutralized by vaccination.The statistical language of genetics is certainly a maze to the uninitiated, but the logic is ultimately on the common sense level.
So, let's be clear:
- This graph tells us that the SARS-CoV-2 samples from highly vaccinated nations are more similar to one another than are those from less vaccinated nations. The obvious conclusion is that the self-similar viral pools are more likely to be vaccine resistant.
- This graph does not tell us that the rate of mutation (SNPs per generation) changes in any way. In fact, that rate likely does not to any appreciable degree, though I suspect that many readers confirming their media-seeded "unvaccinated are variant factories" biases interpret it that way.
Note that when selection [for environment] occurs, the genetic variance of the genome "resets" relative to a new baseline because the other branches are "forgotten" in the sense that they are not present in the remaining population. Thus, we get low mutation frequency.
So, the graph on its own is fine. In fact, it's great information! The problem is how the authors [claim to] interpret this information.
They leap---quite incorrectly---to the notion that the suppression of mutation frequency equates to suppression of emergent mutations.Looking back at the introduction, I see a hint that these authors are not particularly deep in the statistical genetics field.
Mutations generate different SARS-CoV-2 variants to escape vaccine-mediated immunity and thereby, develop drug or vaccine resistance
This doesn't really make sense, or is terrible language to describe what is going on. Mutations don't "generate variants
with a purpose". Mutations just happen. They are then selected according to contextual fitness in their environments. Left to random chance (sans vaccine), the locus of genetic diversity can get large, and so in the rare instances a single virion piles up enough SNPs to affect a functional domain (one functional specifically in escaping immunity), it nearly always get outcompeted locally before it can establish itself in another host. Even worse---en route to piling up multiple SNPs, such virions become increasingly unstable (less fit) as per Muller's ratchet.
The authors do not appear to have deep backgrounds in statistical genetics. Had I the free time, I'd read the several other papers the pair co-authored during the pandemic to see if they're all half-baked.
Still, as I said, I am glad to know the information in the paper. While their confusion over the meaning of the information seems consistent, their computations and graphs give us important confirmation about what is really going on. This includes their Tajima's D computations. For those not familiar, Tajima's D is a statistical test conjured by Japanese researcher Fumihiro Tajima to test the "neutral mutation hypothesis". Like my wife sometimes does, Tajima studied mutations in fruit flies (Drosophila).
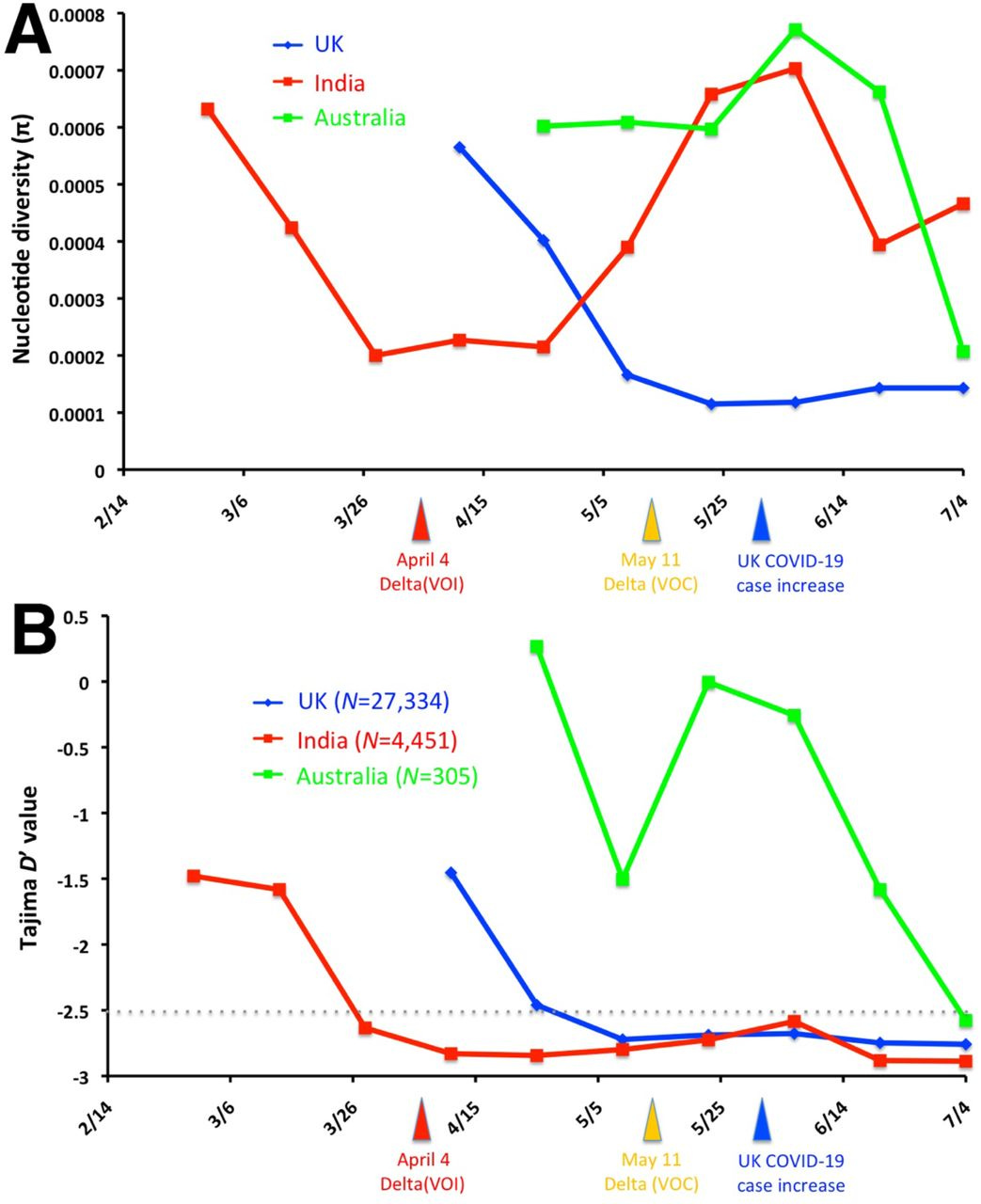
This is the second graph in the paper, and it shows values of Tajima's D that
go negative in India and the UK in particular---just prior to Delta variant breakouts! While I hate to quote Wikipedia, there is a simple table that explains what I noted above about the genomic "resets":

The correct interpretation is that vaccination campaigns channeled mutations through the bottleneck toward their moment of immune escape.
What Are the Implications of This Author Misinterpretation?The problems get substantially compounded by the viral variant of abused reputation. Specifically, Scripps Research Institute founder Eric Topol, a man whose great achievement in genetics was an undergraduate paper opining about prospects for genetic therapy, got ahold of the paper and
tweeted out what looks to be an even worse interpretation than that of the authors: that the result, if true, even as misinterpreted, necessarily generalizes:
@EricTopol
Debunking the myth that vaccination promotes mutations. Being fully vaccinated actually suppresses them
Now Go Do that Doo Doo that You Do So Well
It has grown extremely hard for me to respect Eric Topol on an even basic level. At some point, somebody must have convinced him that if he writes books about futuristic medicine (speculative topics for which nobody has to answer an actual argument beyond, "This will happen in the future,") he'll become fabulously rich and famous, and influence people. Perhaps that experience led him to fool himself into believing that he understands things he does not---like basic math.
And despite being the author of the book Deep Medicine: How Artificial Intelligence Can Make Healthcare Human Again, Topol appeared entirely clueless when interviewed about the world's most obviously fraudulent machine-learning-generated (NEVER HAPPENED) medical research (the Surgisphere paper on hydroxychloroquine's effects on COVID-19 patients).
Now, here he is,
declaring a myth debunked while overgeneralizing an incorrect interpretation of data that says exactly the opposite of what he seems to think it does. And his many thousands of followers have no sense of how little he understands statistics, much less statistical genetics.Predictably, Edward Nirenberg seems to have jumped on the incorrect interpretation as well. Since he is young, with ample opportunity to shed the notion that he understands more than he does (trained to that point no doubt by the educational institutions that fail us all), he has plenty of time to establish a locus of reality. However,
his influential pandemic-era writing reads like a peacock-display of understanding much more than he does while cross-troping Reality Show political phrases like "deplatform [disease]" and "[vaccine] nationalism". Sigh.
I wonder what evolutionary theory he would cite if he cited any.
Sadly, this is how the public winds up being misinformed at about every turn during the pandemic.
Can you imagine how Topol's going to look if the public comes to the conclusion that hydroxychloroquine works and vaccines kill more than help?
https://roundingtheearth.substack.com/p ... t-analysis