Caveat Lector

https://twitter.com/HegKong/status/1491 ... _P9F6r77fw

https://www.bitchute.com/video/sGEtgddwrVSq/
AND:

https://twitter.com/Artytom/status/1490 ... _P9F6r77fw
https://greatgameindia.com/fauci-threat ... ists-aids/
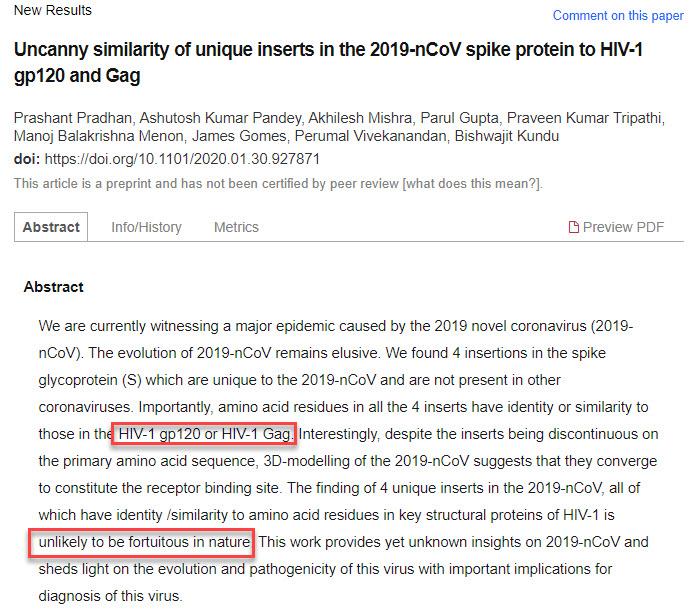
Dr Anthony Fauci Threatened Indian Scientists To Withdraw Study Linking COVID-19 To AIDS Virus
June 6, 2021
https://vaccinedeaths.com/2022-02-04-do ... -aids.html
Doctors are testifying that COVID-19 vaccines are giving people cancer and AIDS
02/04/2022
More individuals fully vaccinated against the Wuhan coronavirus (COVID-19) are developing cancer and even AIDS. This is according to prominent physicians Dr. Ryan Cole and Dr. Vladimir “Zev” Zelenko.
Cole, a board-certified pathologist and owner of a diagnostics lab in Idaho, was called to participate in Wisconsin Sen. Ron Johnson’s Senate panel called “COVID-19: A Second Opinion.”
This discussion panel featured world-renowned doctors and medical experts who were given a chance to provide alternate opinions regarding the experimental and dangerous COVID-19 vaccines. (Related: Fully vaccinated people make up 71% of new cases and 60% of COVID hospitalizations in US.)
Cole, who was originally invited to talk about early at-home COVID-19 treatments, also provided his testimony.
According to Cole, he conducts around 40,000 biopsies a year as a pathologist and he has been seeing more cancers pop up in people who ordinarily would not be susceptible to developing the kinds of cancers he has been seeing. The only similarity between all of these people is that they have all been vaccinated.
Cole collected all of his data and attempted to contact other laboratories to aggregate a bigger dataset. For pointing out what he has observed, Cole said he was ridiculed and maligned.
“I have oncologists, I have radiation oncologists [tell me] ‘I am seeing an uptick in cancers,’ ‘I’m seeing these odd stable cancers take off like wildfires after the vaccines,'” said Cole. “It is happening. We need federal funding. The NIH [National Institutes of Health] isn’t looking at this. Getting a grant to look at anything related to the vaccines is next to impossible.”
This is not the first time Cole has spoken about the rise in cancers among those vaccinated against COVID-19. In Sept. 2021, Cole went viral after a video of him talking about seeing a rise in cancers and autoimmune diseases among the fully vaccinated was made public.
“Since Jan. 1 [2021], in the laboratory, I’m seeing a 20 times increase of endometrial cancers over what I see on an annual basis,” said Cole in the video. “I’m not exaggerating at all because I look at my numbers year over year. I’m like, ‘Gosh, I’ve never seen this many endometrial cancers before.'”
Vaccine’s immunity-killing properties cause immune deficiency problems among the fully vaccinated
On Jan. 11, Zelenko, a Ukrainian-American family physician, was interviewed by Clay Clark, host of the Thrive Time Show on Brighteon.TV to talk about how the fully vaccinated patients he has been seeing are experiencing immune deficiency problems.
“They have AIDS. But it’s not HIV-induced AIDS,” said Zelenko. “HIV damages your killer T cells and weakens your immune system. So, that syndrome is called AIDS. But there are other things that damage your immune system.”
“By taking a shot that damages your natural killer T cells, damages your tumor suppressor genes, what’s happening is your innate immune system is getting shot,” he continued.
Zelenko then explained that this “vaccine-acquired immunodeficiency syndrome” is the reason that he and many other doctors have seen a massive surge in debilitating illnesses like cancer, autoimmune diseases and other “opportunistic infections” and conditions like heart attacks, strokes and miscarriages.
Ben Armstrong, a journalist working for the New American pointed out on his show, “The Ben Armstrong Show,” that all of this information blows up the entire narrative people have been fed regarding the COVID-19 vaccines. His hope is for this kind of information to be aired worldwide so that more people can see it.
“But of course, that’s never going to happen. That’s a pipe dream,” he said. “So, we’ll have to push it out grassroots style, as we’ve been doing with the truth the whole time. It’s always through the grassroots, [through] people like you spreading this type of information.”
Viability and corroboration TBD, though the recent DoD whistleblower allegations align with the above:
Pentagon Responds To DoD Whistleblowers' Claim Of Spiking Disease Rates In The Military After COVID Vaccine Mandate
Three United States military doctors have blown the whistle on documents allegedly from The United States Department of Defense (DoD) that they had access to, which show “skyrocketing rates of disease” since the introduction and mandating of the virus vaccines in armed forces, human rights attorney Leigh Dundas told The Epoch Times.
Dundas was recently approached by Dr. Samuel Sigoloff, Special Forces flight surgeon Lt. Col. Peter Chambers, and Aerospace occupational medicine specialist Lt. Col. Theresa Long.
They handed documents to Dundas, who appeared recently with attorney Tom Renz in a five-hour hearing organized by Sen. Ron Johnson (R-Wis.) titled “COVID-19: Second Opinion.”
Renz shared some of the numbers related to medical disorders in the U.S. military data with The Epoch Times.
The whistleblowers, who are represented by Renz, gave him the data “under penalty of perjury,” he said during the hearing.
Renz intends to submit the information to the courts, he told Johnson.
...
Renz responded:“The DoD has claimed that the DMED data from the years 2016-2020 was incorrect. This is absurd. We spend millions of dollars per year on DMED and people monitoring DMED which is one of the premier epidemiological databases in the world. Accuracy in this database is critical as it is used to monitor for health issues in our troops.
https://www.zerohedge.com/covid-19/pent ... fter-covid
Yes, it's Zero Hedge and Epoch Times. So it grants the easy option of dismissal.
Time, however, has a way of distilling truth. It may be years from now. But it'll arrive eventually. Hopefully soon.