Analysis of an important new paper just published in ScienceThe first study was published in
Science Immunology on December 22nd, titled
“Class switch towards non-inflammatory IgG isotypes after repeated SARS-CoV-2 mRNA vaccination.” We’ll call this the “December study.” Basically, it ominously suggests that vaccinated people may be developing a systemic tolerance for toxic spike protein.1
The first principle is that there are different KINDS of antibodies, which are used by the human body to handle different kinds of threats. This is similar to how we use different types of military: local police, Border Patrol, Navy, Marines, Army, and so on. The antibodies have shorthand names, like IgA, IgD, IgM, IgE, and IgG. That last one, IgG, has four subtypes, numbered IgG1 through IgG4.
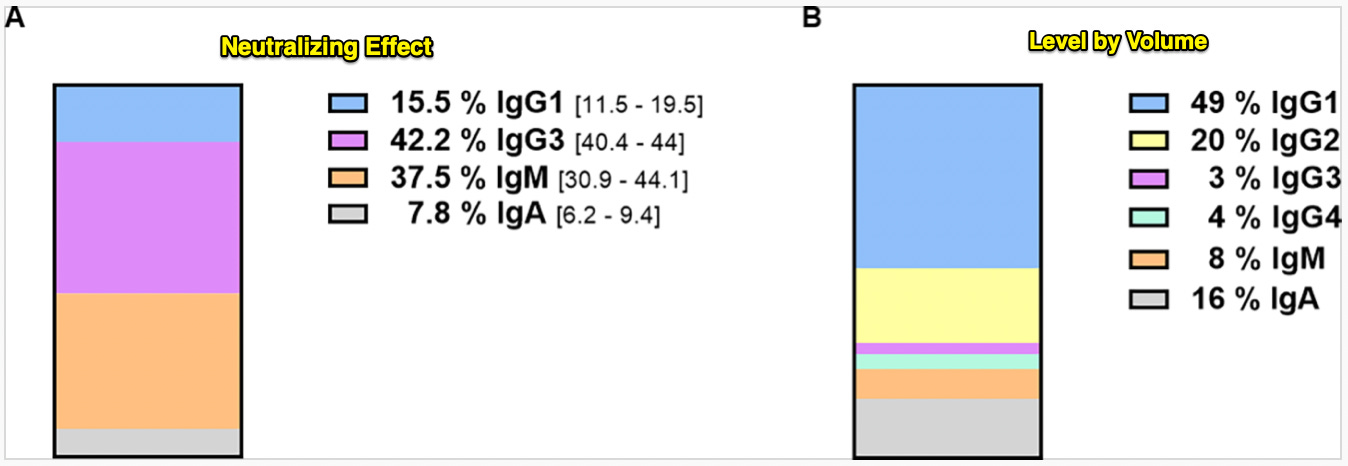
With me so far? Here’s a chart showing the normal, desired immune response to a respiratory virus, by antibody type:
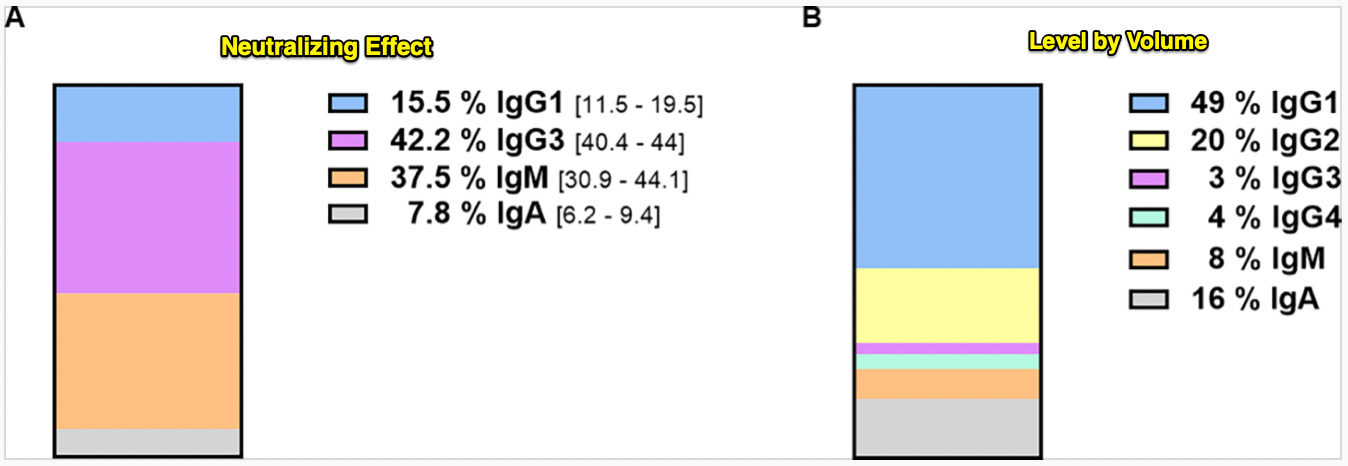
The left side shows how active each of the antibody types were, which is called “neutralizing effect,” because the antibodies “neutralize” the virus. You’ll see two antibody types doing most of the work: IgM (37.5%) and IgG3 (42.%).
On the right side of the chart, you see the amount (volume) of antibodies found in the serum. Interestingly, IgM (8%) and IgG3 (3%) are only present in small amounts by volume, yet as we can see from the left side, are still doing most of the work neutralizing the virus.
The unsurprising takeaway is: The TYPE of antibody is way more important than how much antibody there is. In this case, the body needs the IgM’s and IgG3’s to neutralize respiratory viruses.
But note there is NO neutralizing role for the IgG4 antibody, even though some of it (4%) is still found in the body. There’s a reason IgG4 does not appear in the neutralizing group; we’ll get to that in a minute.
First, here’s a timeline chart showing how IgM and IgG3 work together to help people recover from a covid infection.
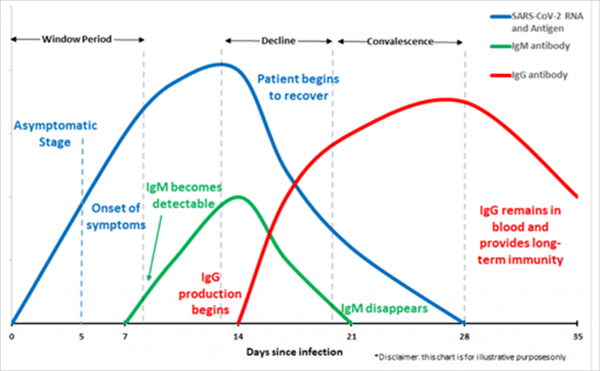
The chart shows that, shortly after symptoms begin, the body starts making IgM. As IgM peaks, the patient begins to recover, and IgM starts to disappear. At about the same time IgM peaks, the body starts making IgG, which then hangs around in the blood providing long-term immunity to the virus.
IgM is like the Marines, which come in first to defeat the rebel army. IgG is more like well-armed local police, who stay behind to keep the peace after the territory has been occupied.
One reason IgM is the type that defeats the virus is that, unlike IgG, it is produced in the mucus membranes, where respiratory viruses flourish. We’ve learned that the covid jabs do NOT spur production of IgM, which is one big reason why they failed to stop the transmission and why breakthrough infections occur.That the jabs spur IgG but don’t increase IgM means the IgG type has to do work it wasn’t designed for in people who’ve never been infected. It’s like sending beat cops to fight the rebel army. They can win, given enough of them, but it’s not the best strategy.
Still, you fight with the army you have, not the army you wish you had. The trouble is, not just ANY type of IgG will work; the body needs neutralizing IgG3. And this is where the jab locomotives really start flying off the rails.You’d think the FDA would’ve made Pfizer measure IgM and IgG3 antibody levels, and not just general antibody levels. You’d think a lot of things, like unicorns, and like pots of gold at the end of rainbows. But it’s not just that they measured the wrong antibodies.
The new studies appear to show that repeated jabs are somehow SUPPRESSING IgG3 antibodies, forcing the body to try to compensate with types not designed for respiratory viruses.It’s like taking the cops’ assault rifles away, making them fight with one-shot pistols, improvised spears, sharpened garden tools, and harsh language.
Now meet IgG4, the antibody the December study found was increasingly present in multiple-jabbed people. The body doesn’t normally use the IgG4 antibody to tackle viruses. That antibody usually handles proteins from allergens like shellfish, bee venom, pollen, and peanuts.In terms of neutralizing capability, IgG3 is up to FIFTY TIMES more effective at neutralizing virus proteins than is IgG4. If IgG3 is a well-armed SWAT team, then IgG4 is Mall Cop.
Here’s the critical first paragraph from the December study:
High levels of neutralizing SARS-CoV-2-antibodies are an important component of vaccine-induced immunity. Shortly after the initial two mRNA vaccine doses, the IgG response mainly consists of the pro-inflammatory subclasses IgG1 and IgG3. Here, we report that several months after the second vaccination, SARS-CoV-2-specific antibodies were increasingly composed of non-inflammatory IgG4, which were further boosted by a third mRNA vaccination and/or SARS-CoV-2 variant breakthrough infections. IgG4 antibodies among all spike-specific IgG antibodies rose on average from 0.04% shortly after the second vaccination to 19.27% late after the third vaccination… Importantly, this class switch was associated with a reduced capacity of the spike-specific antibodies [IgG1 and IgG3] to mediate antibody-dependent cellular phagocytosis and complement deposition.
In study subjects with breakthrough infections, it was even worse: On average, subjects who had a breakthrough infection after their booster shots showed 42.45% IgG4 — almost half. Remember — IgG4 is not even seen in the normal immune response to covid in unjabbed people.Critically, all the vaccinated subjects’ IgG3 levels fell to ZERO (0%) after their third jab in the study. That’s not good.In other words, the researchers found as time goes on, vaccinated people relied more on IgG4 — the allergy antibody — than virus fighter IgG3, whereas it was the exact opposite for unjabbed people. Something seems to be suppressing IgG3 in jabbed people, and the body appears to be compensating by recruiting the available but imperfect IgG4 type.
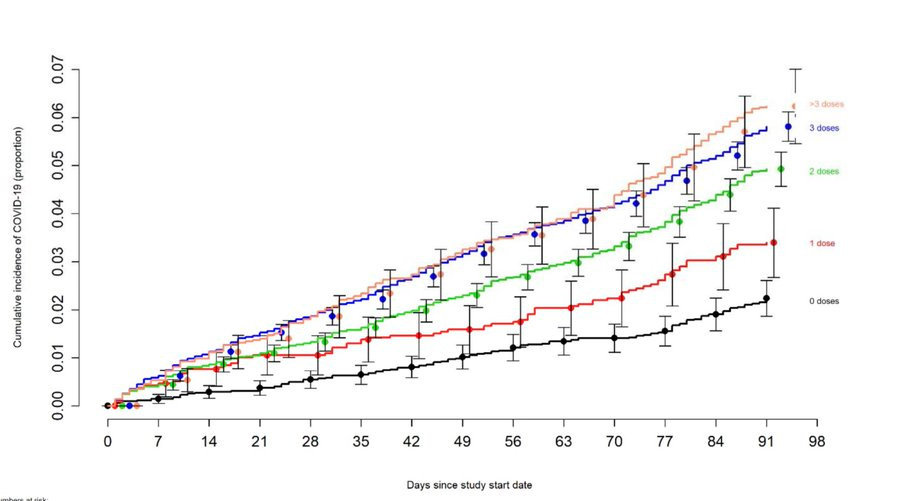
That phenomenon could help explain the expert-baffling chart we saw last week from the Cleveland Clinic study, which found that jabbing increased the risk of reinfection.
It could also help explain this November headline from our friends at The Washington Post:

The Atlantic article, referring to the now-famous Kaiser Foundation study, described what it understatedly called a “troubling trend”:
For the first time, a majority of Americans dying from the coronavirus received at least the primary series of the vaccine. Fifty-eight percent of coronavirus deaths in August were people who were vaccinated or boosted… a continuation of a troubling trend that has emerged over the past year. As vaccination rates have increased and new variants appeared, the share of deaths of people who were vaccinated has been steadily rising. In September 2021, vaccinated people made up just 23 percent of coronavirus fatalities. In January and February this year, it was up to 42 percent.
Twenty-three percent, forty-two percent, now fifty-eight percent. Of DEATHS. And there is no reason to think the trend has peaked yet. This is exactly what you’d expect to see if the IgG4 theory is correct.
In other words, the increasing death rate in boosted people could be explained by the December researchers’ finding that both IgG1 and IgG3 antibody types are being steadily replaced in the vaccinated by the IgG4 type. Returning to the first chart, we saw that IgG1 (15.5%) and IgG3 (42.2%) together did most of the virus-fighting work (57.9%), while IgG4 was nowhere in the list of neutralizing antibodies at all:
 To put it simply, this antibody class shift is bizarre, unprecedented, and a very troubling sign that vaccinated people — especially repeatedly dosed people — are somehow losing their IgG1 and especially IgG3 response in favor of IgG4. It’s not just the reduction of the two effective neutralizing antibody types, either. IgG4, since it is designed for allergies, doesn’t remove the foreign proteins so much as teach the body to “tolerate” or “ignore” them.
To put it simply, this antibody class shift is bizarre, unprecedented, and a very troubling sign that vaccinated people — especially repeatedly dosed people — are somehow losing their IgG1 and especially IgG3 response in favor of IgG4. It’s not just the reduction of the two effective neutralizing antibody types, either. IgG4, since it is designed for allergies, doesn’t remove the foreign proteins so much as teach the body to “tolerate” or “ignore” them.There’s a good reason for tolerance: allergens don’t replicate like viruses. Allergens are a totally different kind of threat. With allergens, the body doesn’t need to go crazy fighting allergens; it can take a slower, more measured response.
Specifically, whereas IgG1 and IgG3 types are “pro-inflammatory,” which means they trigger the body’s immune-system high alert system, the IgG4 type is “anti-inflammatory,” which means it tells the immune system to stand down. Which is the opposite of what you really want, when you’re fighting an infection.The December researchers explained that after the third booster, IgG3 levels fell almost to zero, while IgG4 levels became the second-most dominant antibody type:
Ten days after two immunizations, anti-spike specific antibodies of the isotypes IgG1, IgG2 and IgG3 were readily detectable, whereas anti-S IgG4 antibodies were completely undetectable (Fig. 1C). IgG2 levels were markedly lower than IgG3 and IgG1 levels. Intriguingly, 210 days after the second immunization, the levels of spike-specific IgG4 antibodies exceeded the lower limit of quantification in the sera of about half of the vaccinees. The levels for all other isotypes dropped significantly as expected from the overall anti-S response. While IgG1 was still the most dominant isotype, IgG3 levels fell below the lower limit of quantification. After the third immunization, the amounts of IgG1 were elevated again and reached levels as measured shortly after the second vaccination. Notably, a marked increase in IgG4 antibody levels was observed after the booster immunization in nearly all vaccinees. In some individuals, IgG4 became the second most abundant isotype among the anti-S antibodies
The result was that jab-produced antibodies don’t work as well as natural antibodies at clearing the virus:
{Blood} sera taken after the third vaccination and normalized to the amount of anti-spike antibodies yielded significantly lower phagocytic scores than sera from the same donors after two immunizations.
“Phagocytic scores” refers to how effective antibodies are at neutralizing a virus. Phagocytosis is the process whereby killer cells “eat” virus proteins flagged by antibodies, thereby neutralizing (killing) them. Lower phagocytic scores means the IgG4 antibodies in vaccinated people were less effective at removing the virus than the IgG1+IgG3 types in the unjabbed.
Other studies appear to confirm a misfiring immune response. A November 22nd study published in Frontiers in Microbiology was titled, “Conserved longitudinal alterations of anti-S-protein IgG subclasses in disease progression in initial ancestral Wuhan and vaccine breakthrough Delta infections.”
Similar to the December study, these researchers found higher ratios of IgG4 were associated with more severe disease, and people who had high levels of IgG4 antibodies relative to IgG3 had worse clinical outcomes, meaning they got sicker.
Hopefully, they also found that the antibody ratios between injected and uninjected had stablized six months following injection, suggesting the potential for recovery.Next, a July study published in the New England Journal of Medicine was titled, “Duration of Shedding of Culturable Virus in SARS-CoV-2 Omicron (BA.1) Infection.” The data from the study showed that boosted subjects cleared the virus more slowly than unvaccinated people:
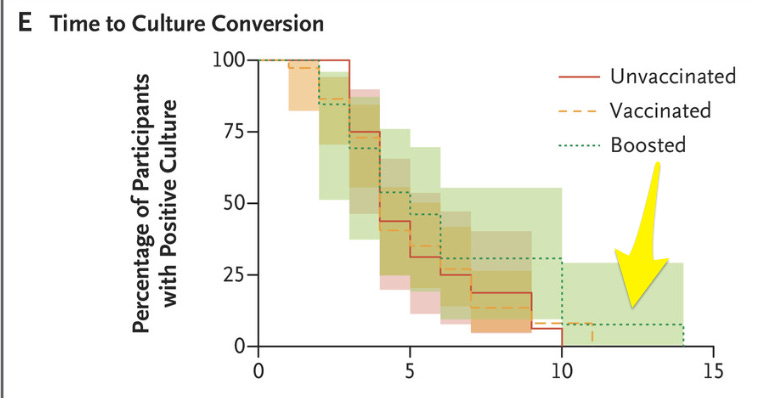 The study data showed the share of boosted subjects who were still contagious (31%) at day ten was over five times more than the share of still-contagious unvaccinated subject (6%). In other words, out of 100 boosted people who catch covid, 33 will still have live, transmissible virus on day 10. Whereas out of 100 unvaccinated persons, only six still test positive on Day 10 — more than five times fewer.
The study data showed the share of boosted subjects who were still contagious (31%) at day ten was over five times more than the share of still-contagious unvaccinated subject (6%). In other words, out of 100 boosted people who catch covid, 33 will still have live, transmissible virus on day 10. Whereas out of 100 unvaccinated persons, only six still test positive on Day 10 — more than five times fewer.
Not only are the boosted dying in increasing numbers, but they are carrying the virus longer. Houston, we have a problem.The unknown is the most troubling part. Nobody has any idea what happens after artificial disruption of a large part of the population’s immune response. We can reasonably assume we’ll see increasing covid infections for boosted folks. Another troubling possibility is that other viruses could begin to evolve to take advantage of the reduced IgG3 response in boosted people, making new variants targeting boosted people.
A wild but troubling possibility appeared in another research article published in August in the Yemen Journal of Medicine, titled “Immunoglobulin G4-related disease: A narrative review.” Here’s the first paragraph:
Immunoglobulin G4-related disease (IgG4-RD) is a new and evolving immune-mediated disease characterized by focal or diffuse organ infiltration by immunoglobulin G4-bearing plasma cells which, if left untreated, leads to irreversible fibrosis, organ dysfunction, and death… IgG4-RD can affect any organ in the body with a variety of clinical features that mimic malignant, infectious, and inflammatory conditions, making diagnosis difficult. Therefore, a high index of suspicion is necessary for the early detection of this disorder, to avoid irreversible damage and death.
This baffling new syndrome is poorly understood, but diagnosis includes measuring serum IgG4 levels, which appear high in people who have the novel disease. So it appears sustained high IgG4 levels may be a bad sign. Fortunately, the novel syndrome remains rare and there’s no evidence connecting it to the vaccines. Not yet.
The point is, we have no idea at all what the result of IgG3 suppression and IgG4 promotion might be. Still, the good news is that we’re finally learning more about the actual mechanisms behind the problems. That’s good news for accountability, and it’s good news for vaccine-injured people, because it is also the first step toward effective treatments.
Most vaccine recipients are victims. They were manipulated or coerced into taking something without informed consent, a drug pushed by reassuring government agencies, agencies they had every reason to trust, because they paid good tax money to over-fund those agencies and handsomely reward the bureaucrats running them.
We need to both help the victims as well as bring accountability to the culpable.