Surprise, surprise, surprise!!!
New South Wales Health erased Covid, vaccine data used in weekly reportsLike many Australians cooped up during Covid lockdowns, Xin Yin Ooi found herself “obsessed” with weekly updates from health authorities, poring over case numbers, vaccinations, hospitalisations and deaths.
As a data analyst, the Sydney woman was naturally interested in the detailed statistical breakdowns provided in NSW Health’s weekly surveillance report — so when she noticed a strange figure in one table, she decided to request the underlying numbers to check the work for herself.
The only problem? The data had been “erased”.
“It was a big shock,” Ms Ooi said.
“In the early days of Omicron, our Premier, Health Minister, chief health officer, every day at the press briefing I remember vividly they were saying, ‘The data shows two doses are not enough, you need three to deal with Omicron.’ They kept repeating, ‘the data, the data’ — it’s just unbelievable they would erase the data.”
Earlier this month, the NSW Civil and Administrative Tribunal (NCAT) ruled in favour of NSW Health in a freedom-of-information battle with Ms Ooi, who first lodged a Government Information Public Access (GIPA) request with the agency more than a year ago.
‘Long journey’
Ms Ooi had asked NSW Health to provide “patient level de-identified data” which underpinned two tables in the surveillance report published in the first week of February 2022.
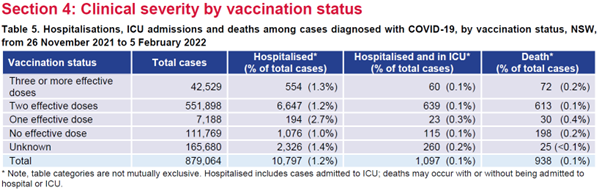
Table five of that report was a breakdown of hospitalisations, ICU admissions and deaths between November 26, 2021 and February 5, 2022, sorted by vaccination status — one, two, or three or more “effective doses”, no “effective dose” or unknown.
Table six was the “proportion of cases with a severe outcome” of either ICU or death, broken down by age and vaccination status — but only showing “three or more effective doses”, “two effective doses” or “less than two effective doses”.
Ms Ooi also requested any “other relevant info that can help me understand this data”, saying in her March 2022 application that “my first analysis objective is to ungroup the last two columns on table six into [a] more refined vaccination category”.
“This is actually a very important table — it traces the cases since Omicron arrived in NSW, it was a new virus at the time, everyone wanted to know what it does,” she said.

“What is interesting is you actually see, moving from no dose to one dose, there is actually an increase [in hospitalisation] from 1 per cent to 2.7 per cent if you look at that column. I’m a data analyst by profession, I wanted to know why, so I did a GIPA. That started my long journey pursuing this.”
https://threadreaderapp.com/thread/1659 ... 66400.html1. It appears that at least in NSW, the Covid vaccination program has not included collecting data to check and verify that the vaccines works. NSW Health produced tables like this in its weekly Covid-19 Surveillance Reports without saving the data used.
2. This is another format of the table that used the same data extracted each week. Not a single record of the data has been saved by NSW Health, according to: Ooi v NSW Ministry of Health [2023] NSWCATAD 107:
https://www.caselaw.nsw.gov.au/decision ... 5e161bac7#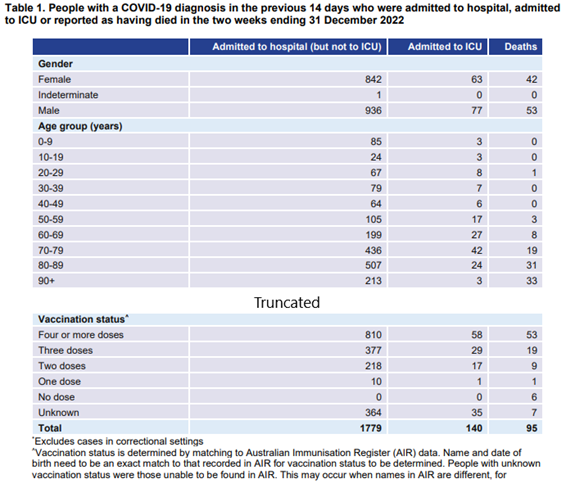
3. I want to preface by saying I’m not here to bash NSW Health, I revere the men and women who work for this organisation, who keep our health system going.
4. In 2021, our government told us that Covid-19 is an unprecedented pandemic that requires an unprecedented solution, which is to vaccinate the entire population with few exceptions…
5. … the old, young, middle age, everyone, with Covid-19 vaccines that have just gained provisional approval from the TGA.
6. They told us that this is our way out of the pandemic. That the vaccines will ‘stop the spread’. Later, our government said even if vaccination doesn’t stop the spread, it will make us less likely to be hospitalised, end up in the ICU, or die.
7. Logically, NSW Health having led our Covid response, should be very keen (and obligated) to check that the vaccination program works, that it achieves the intended objectives.
8. I put in a GIPA information request on 01 March 2022, demanding the data that is used to compute these tables, with personal information removed (‘de-identified’)
9. These tables are interesting because they show Covid cases from 26 November 2021 - the day that Omicron arrived in NSW. A new virus that was unknown, which magnifies the importance of tracking what it does to patients.
10. I’m a Data Analyst. I know that nearly all tables of figures are created using an underlying dataset. I know that there are established techniques to remove private information (e.g. name, Medicare no.) – hence I asked for de-identified data.
11. NSW Health refused my request, saying that to provide me with this data they will have to create new information that doesn’t exist before, and doing so is too hard.
12. That is strange? What have NSW Health used to produce these tables in the report, if not the data that I asked for?
13. For many times, I've heard our Premier, Minister for Health, Chief Health Officer saying at the daily Covid press briefing, that they follow the data closely, that all data shows that the vaccines work. Surely it includes THIS data?
14. NSW Health said the data I requested has been erased. In other words, it used to exist, but it wasn’t kept.
15. According to NSW Health, “the process of extracting data from each of the sources and linking the data sets was an extremely complex process and took several hours…
16. …Once the data was extracted, an analyst ran the code to create the tables with the outputs which were then reviewed by the epidemiologist. This process took a further several hours.” (from [36] of NCAT decision)
17. “The data” as referred here, is the very information I requested. According to NSW Health, this data “is held within the machine RAM and only exists for the duration of the R [software] session.” (from [37] of NCAT decision)
18. In other words, this data that was the output of hours and hours of work, that we taxpayers pay public servants to do, got erased after the tables are created.
19. According to NSW Health, “Given the time taken to produce the tables, if there were any issues with the information in the tables, the epidemiologist would make changes direct to the tables rather than undertake a re-extraction exercise.” (from [38] of NCAT decision)
20. How could the epidemiologist be confident that the table’s figures are accurate, without referring to a saved record of the underlying data? What are those “issues with the information in the tables” that warrant such unchecked changes?
21. NSW Health said that “the only record resulting from the analysis in R was the final versions of Tables 5 and 6 that are published in the Weekly Reports.” (from [39] of NCAT decision)
22. How strange is this practice of not saving intermediary data and draft tables, when there were multiple people working on data extraction and creating tables, over hours and hours ? And this practice gets repeated week after week.
23. Throughout 2021 and 2022, our government’s main strategy for Covid was the vaccination program that targets people from nearly every age group, including young children.
24. Young children being vaccinated, and Covid sometimes being a long-term disease (think ‘long covid’). Both serve to magnify the need for NSW Health to retain data from one week to another. How else would we know that the vaccines work?
25. Given that hours and hours were spent in producing this data, it is unthinkable that NSW Health will choose to erase this information (that is very valuable for handling an unprecedented pandemic.)
26. For example, NSW Health should at least be curious (!) to learn how a vaccinated patient who is hospitalised, progressed from this week to next week. Or whether vaccinating children makes sense from a clinical risk/benefit angle.
27. Notwithstanding that I asked for de-identified data (i.e. without private information), NSW Health argued that it is not their normal practice to retain this data, because of “privacy concerns”…
28. … whereas the past 3+ years have shown that our government tends to prioritise ‘public safety’ over individual freedom and privacy.
29. Think contact tracing, vaccine passport, workplace vaccine mandates where individual’s movement, private medical information and vaccination status are tracked and stored like never before, by businesses, employers etc.
30. NSW Health wholly owns (and retains) 2 out of 3 data sources it used to construct those tables. The only one it doesn’t own (and retain) is the Australian Immunisation Register that gives vaccination information. (from [35] of NCAT decision)
31. When employers are allowed to retain staff’s vaccination status, NSW Health’s argument that it can’t, for a purpose (pandemic surveillance) that doing so is clearly necessary, is frankly unconvincing.
32. To quote Dr Kerry Chant from a Covid press briefing: “It is important as I read out those deaths and the vaccination status to understand that age and underlying chronic conditions are key indicators of the risk of severe COVID for both hospitalisation and death…
33. … But that data also indicates that vaccines work and can I just reinforce everything that the literature is throwing up, every report that is published, every study shows the benefit of having that booster dose.” (Dr Kerry Chant, 27 January 2022)
34. The data shows that the vaccines work, she said. If NSW Health didn’t save the data used to produce its weekly Covid surveillance reports, what data could Dr Chant be referring to ?
35. If similar data exists elsewhere, NSW Health would still be obligated to supply it to me as per GIPA legislation. NSW Health told NCAT that they did all the searches they could, and didn’t find what I requested.
36. One final thought: if NSW Health doesn’t see the need to retain this data and its intermediary analysis, on Covid severity by vaccination status, and by age groups, are they interested at all in finding out how well the vaccination program works?
37. At the minimum, this is incompetence, or a lack of comprehension of the gravity of the issue. I pray that they didn’t do this deliberately.
38. Just before I end, a few interesting coincidences:
-shortly after my GIPA request on 01 March 2022, NSW Health stopped reporting tables that used data from 26 November 2021 (the date of Omicron’s arrival)…
39. …-in the same month, NSW Health disbanded the old team ‘PHRB’ that was responsible for producing the Covid surveillance reports up to that point (from [30, 31] of NCAT decision)…
40. …-a week after NCAT published its decision (on 05 May 2023), NSW Health’s weekly surveillance report stopped presenting information on Covid hospitalisation, ICU and death (the very subject my data request was about).
41. Last week we bid farewell to the tables that many of us were obsessed with since 2021. The new report format seems to move away from hyper focusing on Covid, to recognising that flu and RSV are equal risk to the vulnerable population, as they always are.
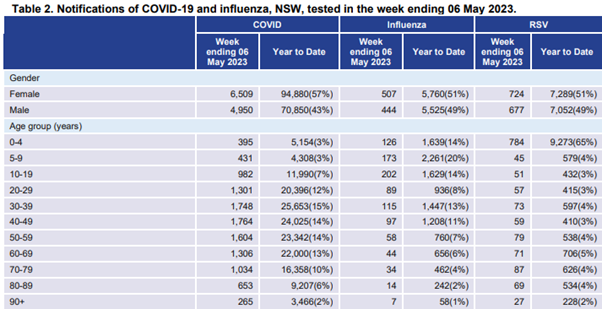
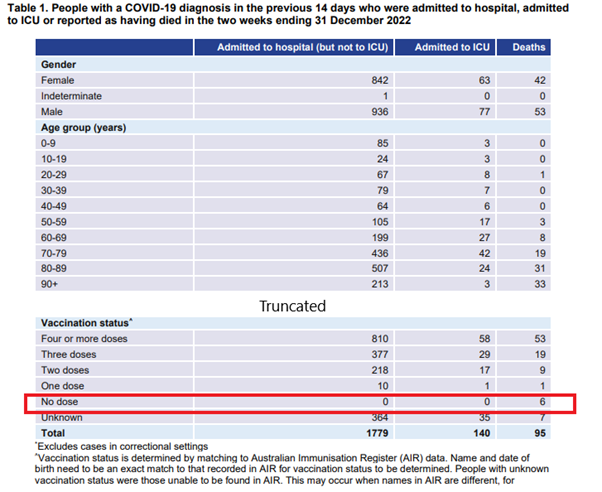
42. As for what the Covid vaccination program achieves: the weekly Surveillance Reports from late June 2022 to December 2022 show extremely low hospitalisation and ICU rate for the unvaccinated population. As the underlying data was never kept, we may never find out why.
The End